All SubjectsAnatomy (1)Anatomy (26)Anesthesiology (9)Biochemistry (26)Community Medicine (10)Dermatology (16)ENT (7)Forensic Medicine (5)General Medicine (1)Internal Medicine (36)Microbiology (23)Obstetrics and Gynecology (13)Ophthalmology (10)Orthopaedics (6)Pathology (1)Pathology (25)Pediatrics (13)Pharmacology (37)Physiology (15)Psychiatry (2)Psychiatry (4)Radiology (11)Surgery (18)
Q11
What are the essential major blood culture criteria for diagnosing infective endocarditis?
Q12
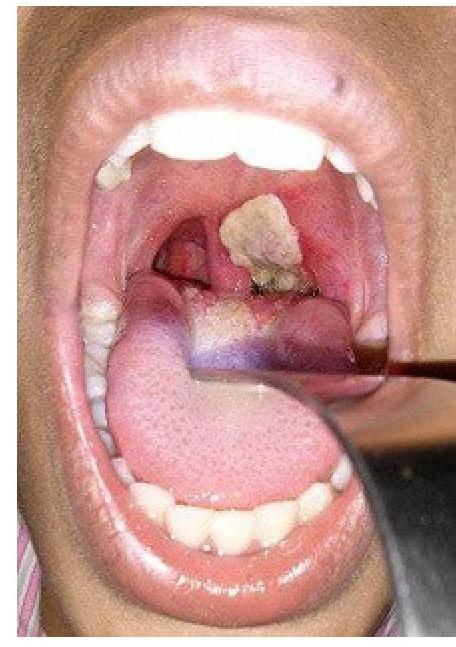
A patient presents with hoarseness of voice and a clinical condition as shown in the image. Identify the lesion:
Q13
Which murmur increases on standing?
Q14
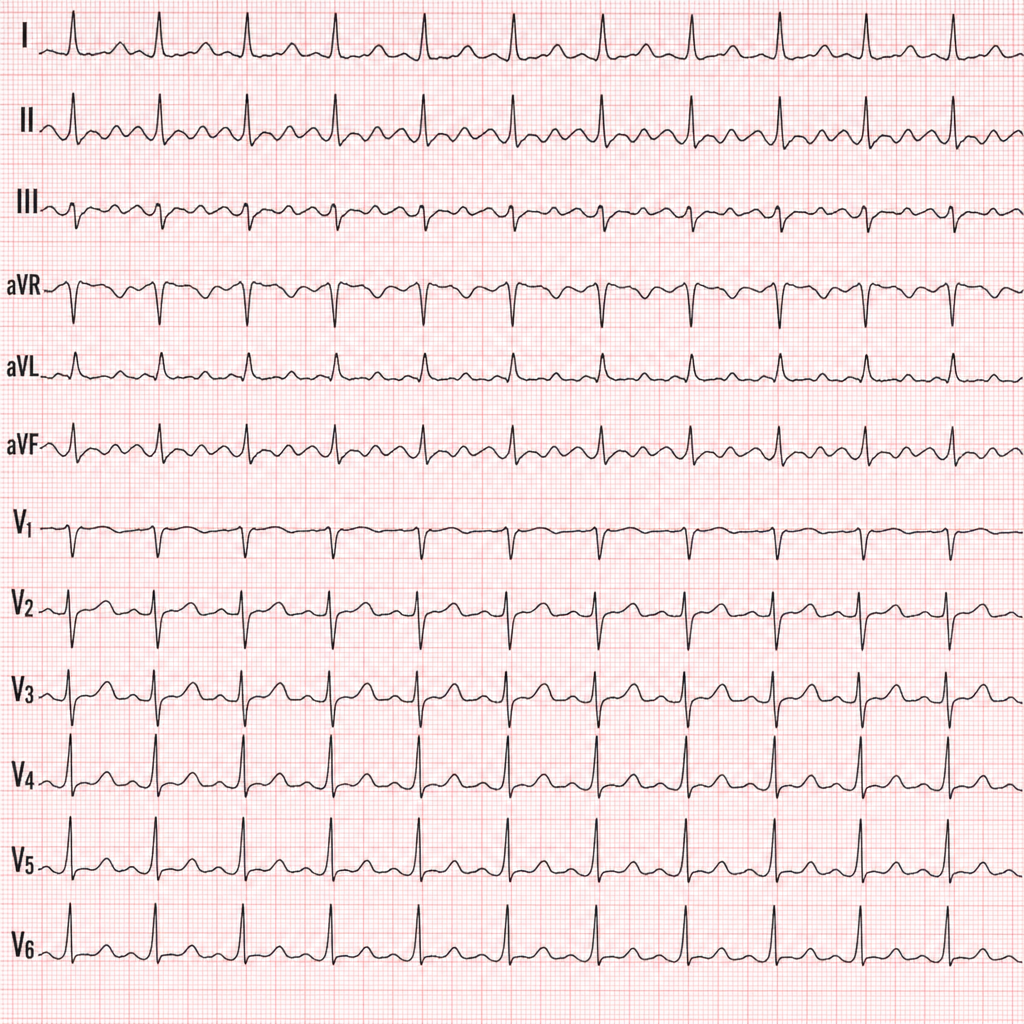
Identify the condition in the ECG based on the provided image.
Q15
Which of the following is a risk factor for Alzheimer's disease?
Q16
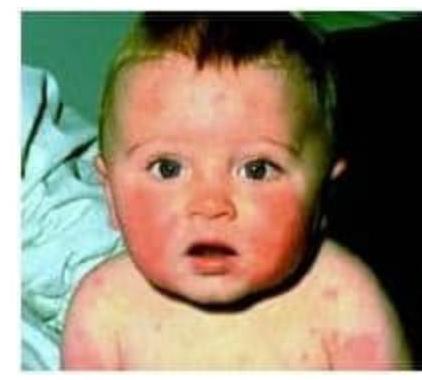
A child with history of fever, photosensitivity, rash sparing nasolabial fold presents to OP. Identify the condition?
Q17
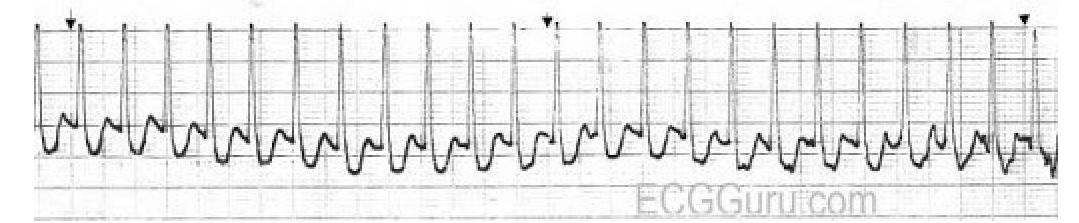
Identify the diagnosis based on the provided ECG image.
Q18
A 65-year-old alcoholic is admitted to the ICU with a diagnosis of acute pancreatitis. After 48 hours, he is unconscious and has the following findings: SpO2= 60%, PO2= 60 mmHg, PCO2=50 mmHg, and HR= 120 bpm. A chest X-ray was performed and is given below. What is the diagnosis of the following condition?

Q19
A 25-year-old female presented to ER unconscious. Her mother tells you about her having recurrent syncopal episodes. Her BP is 80/60 mm Hg and you order an ECG. Treatment is

Q20
Polyuria in adults is commonly defined as urine output exceeding: