All SubjectsAnatomy (1)Anatomy (26)Anesthesiology (9)Biochemistry (26)Community Medicine (10)Dermatology (16)ENT (7)Forensic Medicine (5)General Medicine (1)Internal Medicine (36)Microbiology (23)Obstetrics and Gynecology (13)Ophthalmology (10)Orthopaedics (6)Pathology (1)Pathology (25)Pediatrics (13)Pharmacology (37)Physiology (15)Psychiatry (2)Psychiatry (4)Radiology (11)Surgery (18)
Q11
Which is not correct about the lesion shown below?

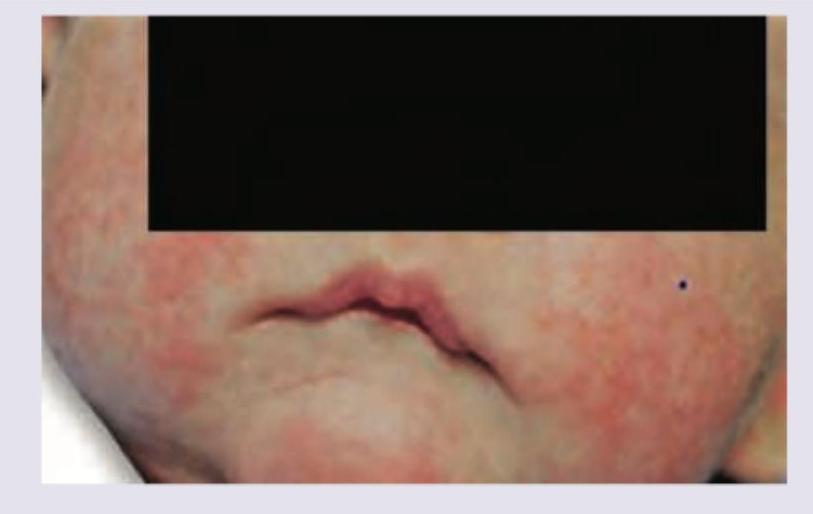
Q12
A one-year-old child presents with the following lesion on the face. His mother has a history of bronchial asthma. What is the diagnosis?
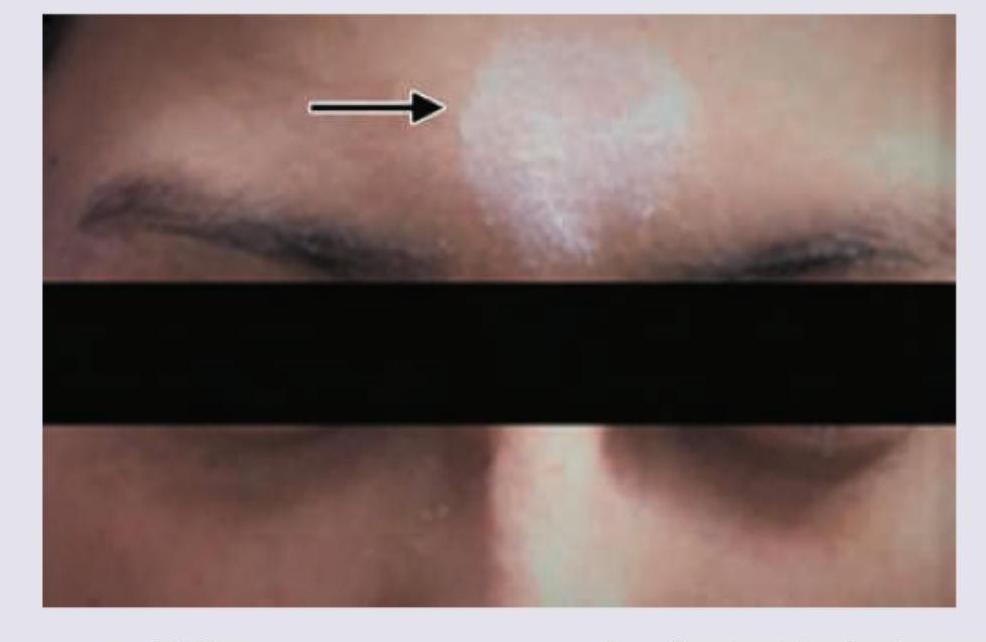
Q13
A patient presents with the skin finding shown in the image. Identify the most likely diagnosis for this lesion.
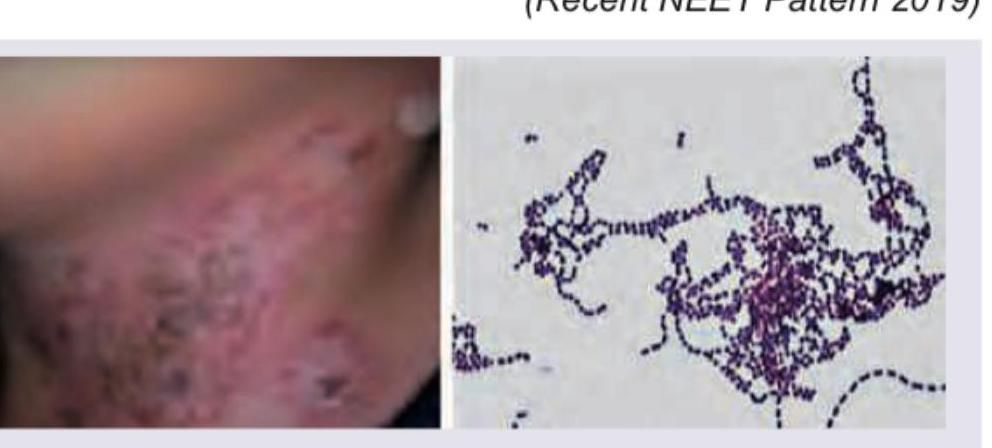
Q14
A child presents with the following lesion in the neck folds. The gram stain from the lesion is shown below. Comment on the diagnosis.
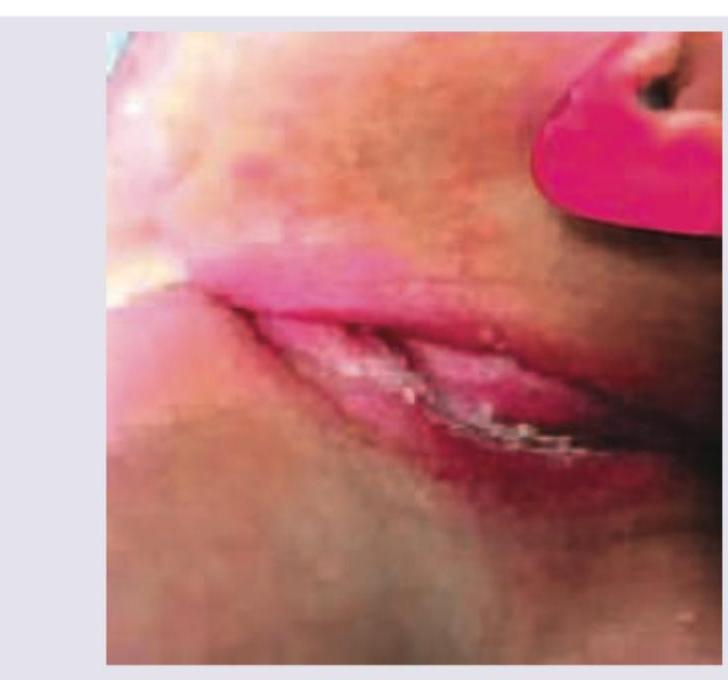
Q15
What is the diagnosis of the lesion visible in neck folds of this child?
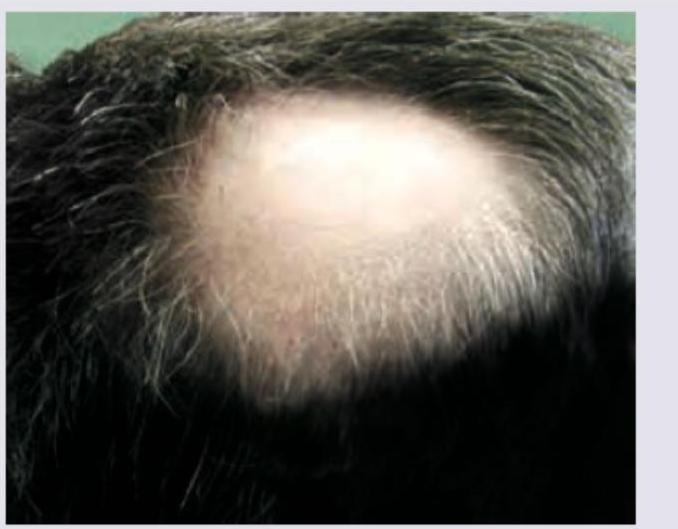
Q16
In a patient with the following lesion on scalp, what changes are seen in the nails?