NEET-PG 2019 — Dermatology
15 Previous Year Questions with Answers & Explanations
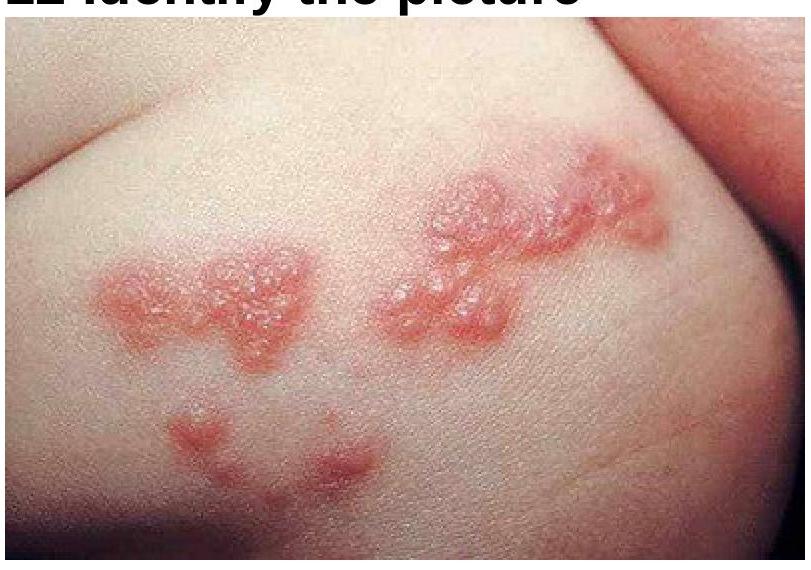
A patient presents with painful vesicular eruptions on one side of the body. What is the most likely diagnosis based on the clinical image?
Identify the condition shown in the image.
A child presents with a rash in the neck folds as shown in the image. The area appears erythematous with satellite lesions and maceration. What is the most likely diagnosis?

Identify the condition in the image

A 26-year-old female patient presented with oral ulcers, sensitivity to light and rash over the malar area of the face sparing the nasolabial folds of both sides. Which of the following is most characteristic of this condition?
All of the following are not true with respect to erythema multiforme except?
The following lesion was noticed in a patient with history of involuntary weight loss. What is the diagnosis?

Which is not correct about the lesion shown below?

A one-year-old child presents with the following lesion on the face. His mother has a history of bronchial asthma. What is the diagnosis?
A patient presents with the skin finding shown in the image. Identify the most likely diagnosis for this lesion.
NEET-PG 2019 - Dermatology NEET-PG Practice Questions and MCQs
Question 1: A patient presents with painful vesicular eruptions on one side of the body. What is the most likely diagnosis based on the clinical image?
- A. Herpes zoster (Correct Answer)
- B. Smallpox
- C. Chickenpox
- D. Atopic dermatitis
Explanation: ***Herpes zoster*** - The image displays characteristic **vesicular lesions** grouped together on an erythematous base, typically following a **dermatomal distribution**, which is classic for herpes zoster (shingles). - These lesions often cause significant pain and are due to the **reactivation of the varicella-zoster virus**. *Smallpox* - Smallpox lesions are typically **deep-seated, firm, round pustules** that are all in the same stage of development. - While smallpox also features vesicular lesions, their appearance and distribution are distinct from the clustered, dermatomal pattern seen in the image. *Chickenpox* - Chickenpox presents as a generalized rash with lesions at **various stages of development** (macules, papules, vesicles, scabs), often described as a "dewdrop on a rose petal." - Unlike the localized, dermatomal pattern of herpes zoster, chickenpox lesions are typically **widespread** over the body. *Atopic dermatitis* - Atopic dermatitis typically manifests as **erythematous, scaly, intensely itchy patches or plaques**, often in areas like the flexural creases. - It does not present with the characteristic **vesicular, grouped lesions in a dermatomal pattern** seen in the image.
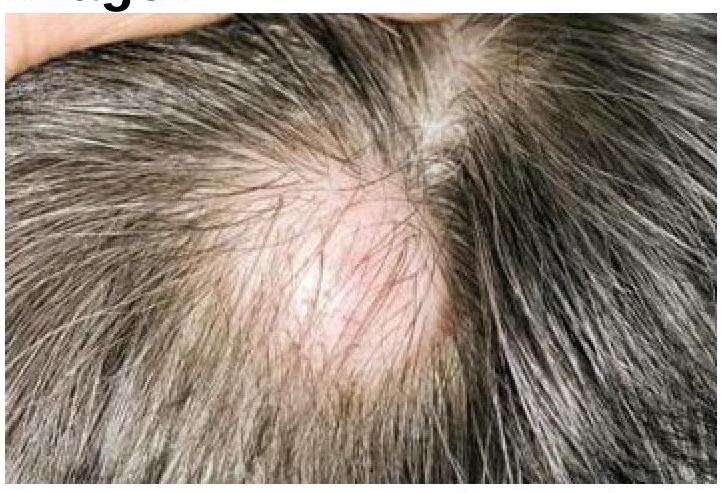
Question 2: Identify the condition shown in the image.
- A. Trichotillomania
- B. Tinea capitis
- C. Alopecia areata
- D. Sebaceous cyst (Correct Answer)
Explanation: ***Sebaceous cyst*** - The image indicates a **well-demarcated, raised lesion** within the scalp, covered by normal skin and surrounded by hair. This appearance is characteristic of a sebaceous cyst (also known as an epidermal or pilar cyst). - Sebaceous cysts are common, benign cysts filled with **keratin** and cellular debris, often arising from hair follicles, and are frequently found on the scalp, face, neck, and trunk. *Alopecia areata* - Alopecia areata typically presents as **smooth, circular patches of complete hair loss** without inflammation or scaling, often described as having "exclamation mark" hairs at the periphery. - The image shows a raised, somewhat erythematous lesion rather than a completely smooth patch of hair loss. *Trichotillomania* - Trichotillomania is a **hair-pulling disorder** that results in irregular patches of hair loss with hairs of varying lengths, often with stubble or broken hairs. - The patches can look bizarre and are usually characterized by hair breakage, not a well-defined raised lesion as seen here. *Tinea capitis* - Tinea capitis is a **fungal infection of the scalp** characterized by scaling, erythema, pruritus, and often broken hairs (black dots). It can also cause pustules and kerions (inflammatory boggy masses). - While it causes hair loss, the primary lesion is usually inflammatory and scaly, rather than a single, raised, non-inflammatory mass.
Question 3: A child presents with a rash in the neck folds as shown in the image. The area appears erythematous with satellite lesions and maceration. What is the most likely diagnosis?
- A. Intertrigo (Correct Answer)
- B. Heat rash
- C. Eczema
- D. Impetigo
Explanation: ***Intertrigo*** - The image shows a reddened, inflamed rash in skin folds (neck creases), which is characteristic of **intertrigo**. This condition results from skin-on-skin friction, moisture, and warmth. - The rash appears to have satellite lesions and a somewhat macerated appearance, which would be consistent with secondary fungal (e.g., Candida) or bacterial infection, common complications of intertrigo. *Heat rash* - **Heat rash (miliaria)** typically presents as small, itchy red bumps or clear blisters, often found in areas prone to sweating. - While it can occur in skin folds, the diffuse, raw-looking erythema and presence of potential satellite lesions shown in the image are less typical for simple heat rash. *Eczema* - **Eczema (atopic dermatitis)** is characterized by dry, itchy, inflamed skin, often with scaling, crusting, or lichenification during chronic stages. - While eczema can affect skin folds, the appearance in the image (intense redness, maceration, potential satellite lesions) is more suggestive of an irritant or infectious process like intertrigo rather than typical eczema. *Impetigo* - **Impetigo** is a bacterial skin infection characterized by honey-colored crusts, vesicles, or bullae, typically appearing anywhere on the body, especially around the nose and mouth. - The rash in the image lacks the characteristic honey-colored crusts or vesiculobullous lesions associated with impetigo.
Question 4: Identify the condition in the image
- A. Leukoderma
- B. Piebaldism
- C. DLE
- D. Vitiligo (Correct Answer)
Explanation: ***Correct: Vitiligo*** - This image shows **patches of depigmented skin** (white areas) characteristic of vitiligo, often seen in a **segmental or generalized pattern**. - Vitiligo is an **autoimmune condition** where melanocytes are destroyed, leading to loss of skin color. - Patches typically have a **progressive course** and can appear at any age. *Incorrect: Leukoderma* - Leukoderma is a **general term** for any condition causing white patches on the skin due to reduced or lost pigmentation. - While vitiligo is a type of leukoderma, this answer is too broad and not the **most specific diagnosis** for the pattern shown. - In clinical practice, we diagnose the specific type (vitiligo) rather than using the generic term. *Incorrect: Piebaldism* - Piebaldism is a **rare genetic disorder** characterized by a **stable white forelock** (unpigmented hair) and often a congenital white patch on the forehead. - Unlike vitiligo, these patches are usually **present at birth** and do not progress. - The distribution pattern is typically **midline** with characteristic forehead involvement. *Incorrect: DLE* - DLE stands for **Discoid Lupus Erythematosus**, which is a chronic autoimmune condition affecting the skin. - It typically presents as **red, scaly, disk-shaped plaques** that can lead to scarring, atrophy, and permanent hair loss. - Would show **erythema, scaling, and scarring** rather than pure depigmentation as seen here.
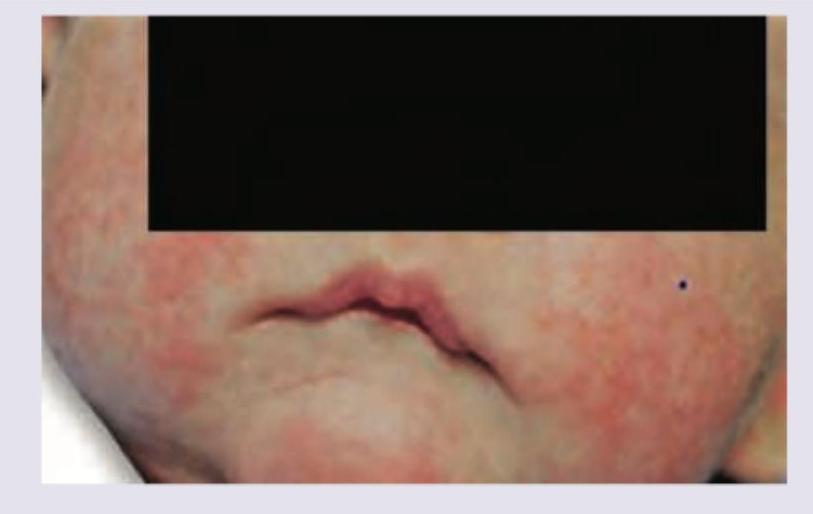
Question 5: A 26-year-old female patient presented with oral ulcers, sensitivity to light and rash over the malar area of the face sparing the nasolabial folds of both sides. Which of the following is most characteristic of this condition?
- A. Butterfly rash sparing the nasolabial folds (Correct Answer)
- B. Heliotrope rash on upper eyelid, bilateral hilar lymphadenopathy
- C. Port-wine stain with CNS malformations
- D. Silvery scales or plaques
Explanation: ***Butterfly rash sparing the nasolabial folds*** - The patient's presentation with oral ulcers, sensitivity to light (photosensitivity), and a rash over the malar area **sparing the nasolabial folds** is highly characteristic of **Systemic Lupus Erythematosus (SLE)**, a condition where a butterfly rash is a hallmark. - This specific distribution of the malar rash is a key diagnostic feature differentiating it from other facial rashes. *Heliotrope rash on upper eyelid, bilateral hilar lymphadenopathy* - A **heliotrope rash** on the upper eyelids is characteristic of **dermatomyositis**, which also presents with muscle weakness, not typically oral ulcers or a malar rash. - **Bilateral hilar lymphadenopathy** is a classic finding in **sarcoidosis**, a granulomatous disease, not directly related to the patient's symptoms. *Port-wine stain, CNS malformations: seen in Sturge-Weber syndrome* - A **port-wine stain** (nevus flammeus) is a congenital capillary malformation, often on the face, and is a principal feature of **Sturge-Weber syndrome**, which involves CNS malformations and seizures. - This condition has no association with oral ulcers, photosensitivity, or the described malar rash. *Silvery scales or plaques: seen in psoriasis* - **Silvery scales or plaques** are the characteristic dermatological lesions of **psoriasis**, a chronic inflammatory skin condition. - Psoriasis typically presents with well-demarcated erythematous plaques and is not associated with oral ulcers, photosensitivity, or a lupus-specific malar rash.
Question 6: All of the following are not true with respect to erythema multiforme except?
- A. Most commonly due to leukemia
- B. Steroids are the drug of choice
- C. Koebner's phenomenon is seen
- D. Targetoid lesions are seen (Correct Answer)
Explanation: ***Targetoid lesions are seen*** - **Erythema multiforme (EM)** is characterized by distinctive **targetoid lesions** (target lesions) with three concentric zones: a dusky center, a pale middle ring, and an erythematous outer ring. - These lesions are a hallmark of EM and differentiate it from many other dermatological conditions. *Most commonly due to leukemia* - **Erythema multiforme** is most commonly associated with **infections**, particularly **herpes simplex virus (HSV)**, rather than leukemia. - Other common triggers include **mycoplasma infections** and certain **medications**. *Steroids are the drug of choice* - For typical, mild **erythema multiforme**, **topical steroids** may be used for symptomatic relief, but they are generally **not the drug of choice** for severe or widespread disease. - **Systemic steroids** are controversial and not routinely recommended for uncomplicated EM, as they may prolong the course or lead to recurrences, though they might be considered in severe cases or to prevent progression to Stevens-Johnson syndrome. *Koebner's phenomenon is seen* - The **Koebner phenomenon** (isomorphic response), where new lesions appear at sites of trauma, is classically associated with conditions like **psoriasis**, **lichen planus**, and **vitiligo**. - It is **not typically seen** in erythema multiforme.
Question 7: The following lesion was noticed in a patient with history of involuntary weight loss. What is the diagnosis?
- A. Acanthosis nigricans
- B. Leser-Trelat sign (Correct Answer)
- C. Actinic keratosis
- D. Intertriginous candida
Explanation: ***Leser-Trelat sign*** - The image illustrates numerous rapidly appearing or increasing **seborrheic keratoses**, which, when accompanied by symptoms like **involuntary weight loss**, are highly suggestive of the Leser-Trelat sign. - The Leser-Trelat sign is a **paraneoplastic syndrome** commonly associated with **gastrointestinal adenocarcinomas** or **lymphoid malignancies**. *Acanthosis nigricans* - This condition presents as **dark, velvety patches** on the skin, typically in body folds like the neck, armpits, and groin. - While it can be associated with malignancy (especially gastric adenocarcinoma), the image shows multiple, distinct seborrheic keratoses rather than diffuse hyperpigmentation. *Actinic keratosis* - Actinic keratoses are **premalignant lesions** caused by chronic sun exposure, appearing as rough, scaly patches on sun-exposed areas. - They are typically single or a few scattered lesions and do not usually erupt rapidly or widely as shown, nor are they directly associated with systemic malignancy in the same way as Leser-Trelat. *Intertriginous candida* - Intertriginous candidiasis is a **fungal infection** that occurs in skin folds, characterized by **redness, itching, and satellite lesions**. - The lesions in the image are distinct, raised, and brownish, not consistent with the erythematous and often moist presentation of intertriginous candidiasis.
Question 8: Which is not correct about the lesion shown below?
- A. The lesions are infectious to seronegative individuals
- B. Can be associated with meningoencephalitis
- C. Bilaterally symmetrical dermatomal vesicular eruption (Correct Answer)
- D. Geniculate ganglion is involved in Ramsay hunt syndrome
Explanation: ***Bilaterally symmetrical dermatomal vesicular eruption*** - The image shows a **unilateral, dermatomal vesicular eruption**, characteristic of herpes zoster (shingles). - Herpes zoster lesions are typically restricted to **one side of the body** and follow a single dermatome, making bilateral symmetry incorrect. *The lesions are infectious to seronegative individuals* - The vesicles of herpes zoster contain **live varicella-zoster virus (VZV)**, which can be transmitted through direct contact. - Individuals who have not previously had chickenpox (seronegative for VZV) can contract **chickenpox** (not shingles) from exposure to these lesions. *Can be associated with meningoencephalitis* - Although rare, disseminated herpes zoster can lead to severe complications, including **meningoencephalitis** if the virus spreads to the central nervous system. - This complication is more likely in **immunocompromised individuals**. *Geniculate ganglion is involved in Ramsay hunt syndrome* - **Ramsay Hunt syndrome (Herpes zoster oticus)** is a specific complication of VZV reactivation involving the **geniculate ganglion** of the facial nerve. - This involvement leads to facial nerve palsy, ear pain, and typical vesicular rash in the ear canal or on the auricle.
Question 9: A one-year-old child presents with the following lesion on the face. His mother has a history of bronchial asthma. What is the diagnosis?
- A. Eczematous dermatitis
- B. Seborrheic dermatitis
- C. Atopic dermatitis (Correct Answer)
- D. Contact dermatitis
Explanation: ***Atopic dermatitis*** - The rash on the face of a one-year-old, coupled with a maternal history of **bronchial asthma**, strongly suggests **atopic dermatitis (eczema)** due to its association with the **atopic triad** (eczema, asthma, allergic rhinitis). - In infants, atopic dermatitis commonly presents as erythematous, scaly, and sometimes **weeping patches** on the face and extensor surfaces. *Eczematous dermatitis* - While atopic dermatitis is a form of eczematous dermatitis, this term is **too broad** and does not specify the underlying cause evident from the patient's history. - Eczematous dermatitis describes a **pattern of inflammation** rather than a specific diagnosis. *Seborrheic dermatitis* - Typically characterized by **greasy, yellowish scales** on an erythematous base, often affecting the scalp (**cradle cap**), eyebrows, and nasolabial folds. - It usually **lacks the strong association with atopy** seen in this case. *Contact dermatitis* - Caused by exposure to an **irritant or allergen**, leading to a localized rash. - The diffuse nature of the rash in the image and the family history of asthma make a specific contact allergen less likely as the primary cause.
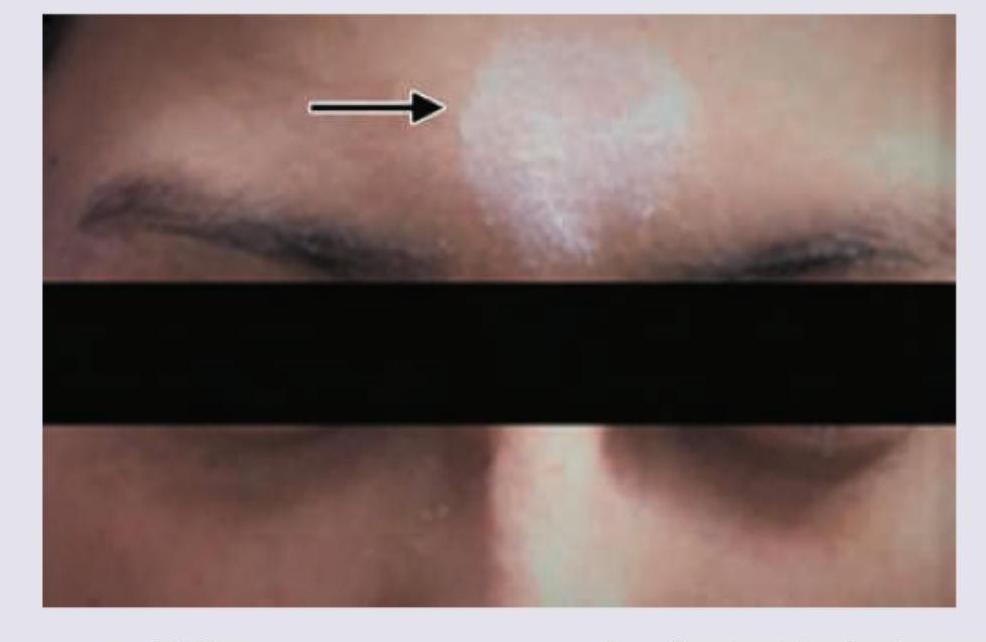
Question 10: A patient presents with the skin finding shown in the image. Identify the most likely diagnosis for this lesion.
- A. Vitiligo
- B. Contact leukoderma
- C. Piebaldism (Correct Answer)
- D. Albinism
Explanation: ***Piebaldism*** - The image shows a **localized patch of depigmentation** on the forehead, characteristic of **piebaldism**. - **Piebaldism** is a rare, congenital autosomal dominant disorder caused by a defect in melanocyte development and migration, resulting in stable, well-demarcated depigmented areas, often with a **white forelock**. *Vitiligo* - **Vitiligo** typically presents as **progressive, acquired macules and patches of depigmentation** that often enlarge over time. - While it can appear on the face, the sharply demarcated, congenital appearance seen here is more consistent with piebaldism. *Contact leukoderma* - **Contact leukoderma** is an **acquired depigmentation** resulting from exposure to chemicals (e.g., rubber, phenols). - It would usually present in areas of direct contact, and the congenital nature of the lesion in the image rules this out. *Albinism* - **Albinism** is a **generalized hypopigmentation** affecting the skin, hair, and eyes due to a defect in melanin production. - The image shows a localized patch of depigmentation, not a widespread lack of pigment characteristic of albinism.