All SubjectsAnatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q11
A 25-year-old patient underwent surgery for scoliosis correction. 5 days post-operatively he develops voluminous bilious vomiting. The given CT abdomen shows:

Q12
Excretory urogram in a two-year-old child with recurrent UTI shows:

Q13
What is the radiological sign that could best describe this image?

Q14
A 26-year-old construction worker with a previous history of recurrent kidney stones presents with flank pain. What is the radiological sign demonstrated in the IVP image shown below?

Q15
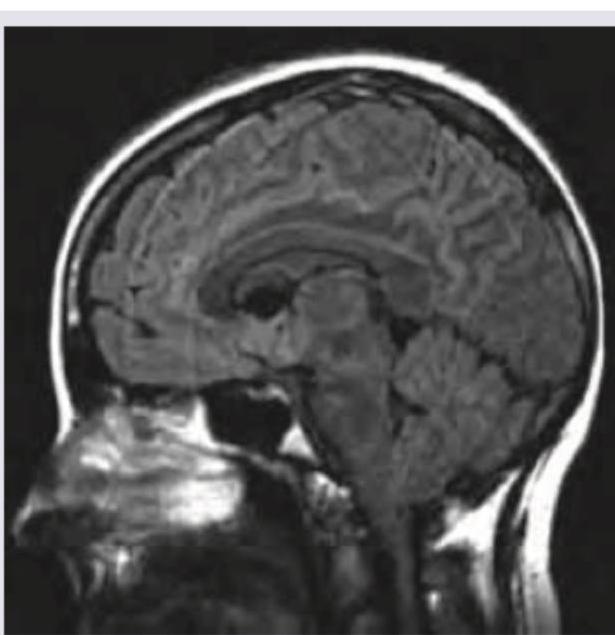
Which of the following is correct about the NCCT shown below? (Recent NEET Pattern 2016-17)
Q16
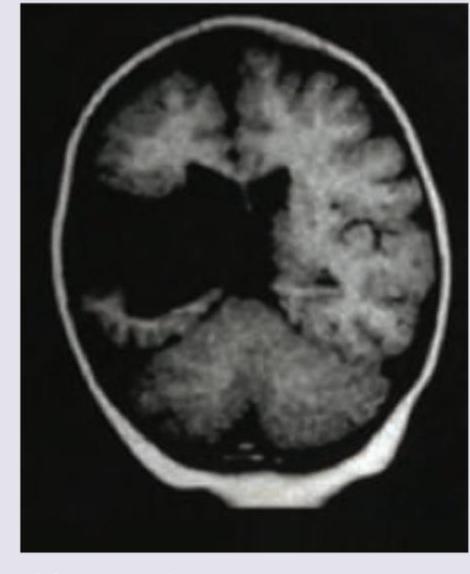
All are true about CNS malformation shown below except:
Q17
A 2-year-old epileptic child with developmental delay presents to emergency with fever for the last two days. NCCT shows:
Q18
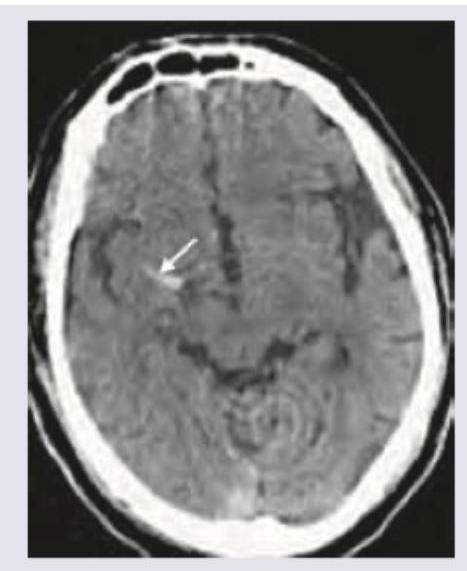
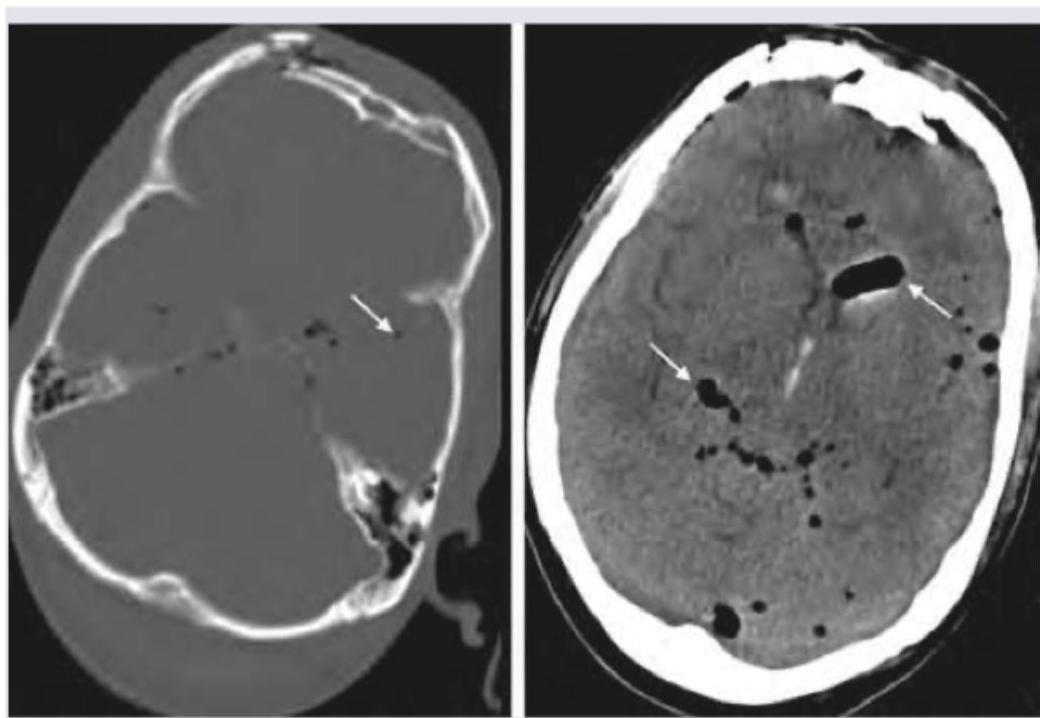
A 79-year-old male presented to the emergency department after a facial trauma. The patient had Parkinson's disease and atrial fibrillation and was on treatment with acetylsalicylic acid for AF. The image shows? (Recent NEET Pattern 2016-17)
Q19
What is the correct diagnosis based on the image shown below?
Q20
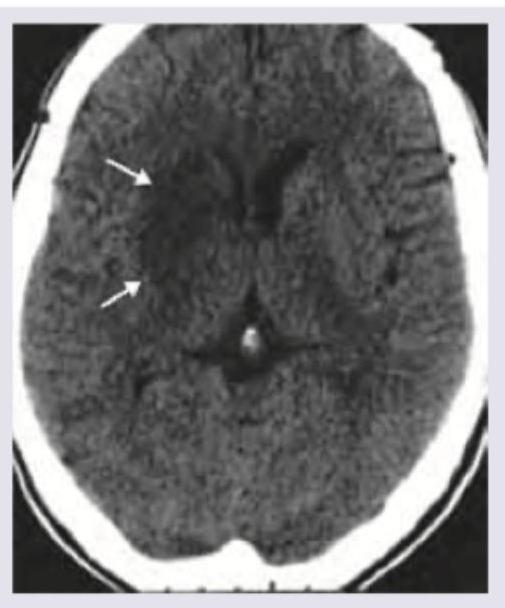
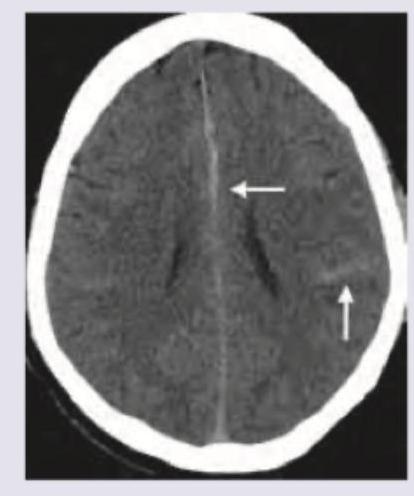
A 55-year-old diabetic patient develops sudden onset hemiparesis and facial asymmetry. NCCT scan shows: