NEET-PG 2017 — Radiology
28 Previous Year Questions with Answers & Explanations
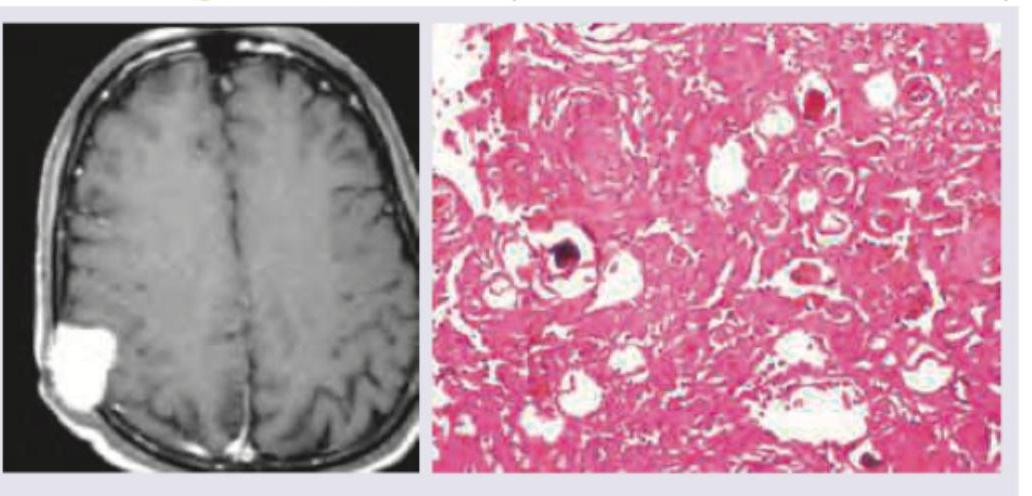
A 50-year-old woman presents with daily early morning frontal headache and projectile vomiting. The image shows:
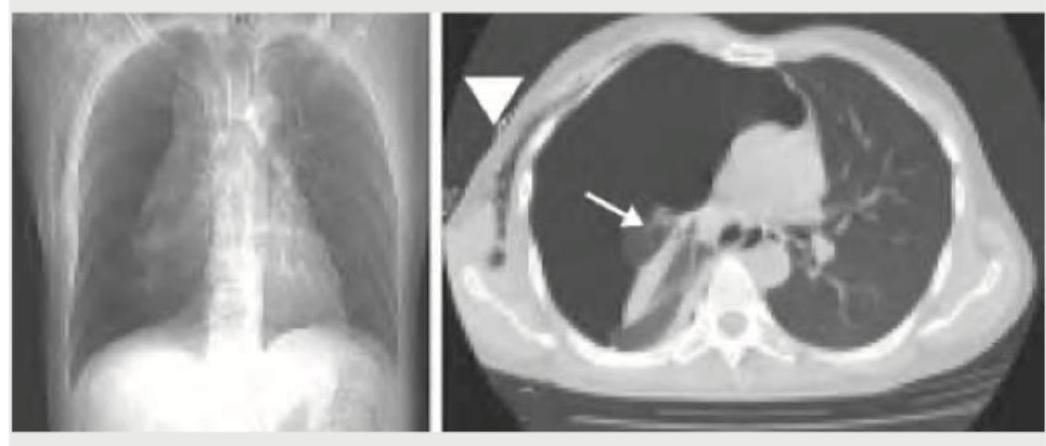
A 40-year-old male presents with sudden onset right-sided chest pain and breathlessness following a road traffic accident. On examination, breath sounds are diminished on the right side. The chest X-ray is shown below. What is the most likely diagnosis?

A chest X-ray shows the following appearance. Identify the pathology:

A 30-year-old hypertension patient presents with daily headaches. The CXR given below shows which of the following? (Recent NEET Pattern 2016-17)

An adult undergoes multiple FFP transfusions for excessive bleeding after cardiac surgery and develops respiratory distress. CXR done is shown below. What does it indicate?

Identify the congenital heart disease presenting with cyanosis in CXR: (Recent NEET Pattern 2016-17)

A breast cancer patient presents with difficulty in breathing. CXR shows:

An AIDS patient presents with respiratory distress. CXR shows:

An 18-year-old boy is brought to the hospital with difficulty in breathing after a bar fight. What does the given CT chest show?
The lung parenchyma on CT chest shown below is best described as:
NEET-PG 2017 - Radiology NEET-PG Practice Questions and MCQs
Question 1: A 50-year-old woman presents with daily early morning frontal headache and projectile vomiting. The image shows:
- A. Medulloblastoma
- B. Glioma
- C. Glioblastoma multiforme
- D. Meningioma (Correct Answer)
Explanation: **Meningioma** - The MRI shows a **well-circumscribed, extra-axial mass** that is significantly enhancing, particularly in the frontal lobe near the convexity. Histopathology of a meningioma characteristically features **whorls of meningothelial cells** and **psammoma bodies** (calcified concentric lamellae), which are visible in the image. - The clinical symptoms of **early morning headaches** and **projectile vomiting** are indicative of **increased intracranial pressure**, which can be caused by any space-occupying lesion, including a meningioma, especially if it grows to a significant size. *Medulloblastoma* - This is a highly malignant brain tumor typically occurring in the **cerebellum of children**, not usually seen in a 50-year-old woman in the frontal lobe. - Histologically, medulloblastomas are composed of small, round, **blue cells** with little cytoplasm (small blue cell tumor), which is distinct from the provided image. *Glioma* - **Gliomas** originate within the brain parenchyma and are often **poorly circumscribed** with an infiltrative growth pattern, which contrasts with the well-defined lesion seen on MRI. - While gliomas can cause increased intracranial pressure, their diverse histological appearances depend on their specific subtype (e.g., astrocytoma, oligodendroglioma), none of which perfectly match the characteristic **whorls and psammoma bodies** seen here. *Glioblastoma multiforme* - **Glioblastoma multiforme** (GBM) is a highly aggressive grade IV astrocytoma, characterized by **ring-enhancing lesions** with central necrosis and significant edema on MRI. - Histologically, GBM exhibits features like **pseudopalisading necrosis**, microvascular proliferation, and pleomorphic tumor cells, which are not depicted in the provided histopathology image.
Question 2: A 40-year-old male presents with sudden onset right-sided chest pain and breathlessness following a road traffic accident. On examination, breath sounds are diminished on the right side. The chest X-ray is shown below. What is the most likely diagnosis?
- A. Hydatid cyst right lung
- B. Right pleural effusion
- C. Right hydropneumothorax (Correct Answer)
- D. Perforated abdominal viscus
Explanation: ***Right hydropneumothorax*** - The X-ray image reveals an **air-fluid level** in the right pleural cavity, characterized by a straight, horizontal line between the air (darker above) and fluid (whiter below). This finding is pathognomonic for a hydropneumothorax. - The **collapsed or compressed lung** is also visible superior to the air-fluid level, further supporting the diagnosis of air and fluid coexisting in the pleural space. *Hydatid cyst right lung* - A hydatid cyst in the lung appears as a **well-defined, rounded opacity (solid mass)**, often with a "water lily" sign if ruptured, but it does not present with a distinct air-fluid level as seen here. - While hydatid cysts can rupture and produce air and fluid, the X-ray findings would typically show a more complex internal structure or a cyst within a cavity, not a simple air-fluid interface across the entire pleural space. *Right pleural effusion* - A pleural effusion would appear as a **homogeneous white (effaced) opacity** blunting the costophrenic angle and, in larger effusions, rising along the lateral chest wall (meniscus sign). - Crucially, a simple pleural effusion **does not show an air-fluid level**; the fluid density would fill the pleural space without an overlying visible air component. *Perforated abdominal viscus* - A perforated abdominal viscus would typically result in **free air under the diaphragm** on an upright chest X-ray (pneumoperitoneum). - While pneumoperitoneum presents as air, it is located below the diaphragm, *not* within the pleural cavity, and would not create an air-fluid level within the lung fields as seen in this image.
Question 3: A chest X-ray shows the following appearance. Identify the pathology:
- A. Pericardial effusion (Correct Answer)
- B. Boot shaped heart
- C. Egg on side appearance
- D. Normal-sized heart
Explanation: ***Pericardial effusion*** - The chest X-ray shows a classic **"water bottle" or "money bag" appearance** with a markedly enlarged, globular, and symmetric cardiac silhouette characteristic of pericardial effusion. - The **clear lung fields** combined with the dramatically increased cardiothoracic ratio indicates fluid accumulation in the **pericardial space** rather than cardiac enlargement. *Boot shaped heart* - A **"boot-shaped" heart (coeur en sabot)** is pathognomonic of **tetralogy of Fallot**, characterized by an upturned cardiac apex and concave pulmonary artery segment. - This appearance results from **right ventricular hypertrophy** and **pulmonary stenosis**, which would show a different cardiac contour than the globular shape seen here. *Egg on side appearance* - The **"egg-on-a-string" appearance** is classic for **transposition of the great arteries (TGA)**, showing a narrow vascular pedicle with an oval cardiac silhouette. - This congenital heart defect presents with **cyanosis in neonates** and has a distinctly different radiological appearance from the symmetric enlargement shown. *Normal-sized heart* - The cardiac silhouette is clearly **markedly enlarged** with a cardiothoracic ratio well above the normal limit of 0.5. - A **normal heart** would have distinct great vessel outlines and proportionate cardiac chambers, not the globular symmetric enlargement demonstrated here.
Question 4: A 30-year-old hypertension patient presents with daily headaches. The CXR given below shows which of the following? (Recent NEET Pattern 2016-17)
- A. Preductal coarctation
- B. Postductal coarctation (Correct Answer)
- C. Aortic dissection
- D. Takayasu arteritis
Explanation: ***Postductal coarctation*** - The image shows **rib notching** (highlighted by the arrow), a classic sign of **collateral vessel development** due to narrowing of the aorta **distal to the ductus arteriosus**. - This congenital heart defect is associated with **hypertension** in the upper extremities and can lead to symptoms like **headaches**. *Preductal coarctation* - This typically presents earlier in life, often with **heart failure** in infancy, and is less commonly associated with **hypertension** and **rib notching** in a seemingly asymptomatic adult. - The coarctation is located **proximal to the ductus arteriosus**, leading to different collateral circulation patterns. *Aortic dissection* - This condition is an acute medical emergency characterized by a tear in the **aortic wall**, often presenting with sudden, severe chest or back pain. - CXR findings typically include a **widened mediastinum**, not specifically rib notching. *Takayasu arteritis* - This is a **granulomatous vasculitis** primarily affecting the aorta and its major branches, leading to narrowing or occlusion. - While it can cause hypertension, **rib notching** is not a characteristic radiological finding; signs usually include vessel wall thickening or stenoses.
Question 5: An adult undergoes multiple FFP transfusions for excessive bleeding after cardiac surgery and develops respiratory distress. CXR done is shown below. What does it indicate?
- A. Volume overloading of heart
- B. Mendelson's syndrome
- C. Pneumomediastinum
- D. TRALI (Correct Answer)
Explanation: ***TRALI*** - The chest X-ray shows **bilateral pulmonary infiltrates** and **pulmonary edema** and the patient had multiple **FFP transfusions** followed by respiratory distress, which is highly suggestive of **Transfusion-Related Acute Lung Injury (TRALI)**. - TRALI is characterized by acute respiratory distress with **hypoxemia** occurring within 6 hours of transfusion, in the absence of other risk factors for **Acute Lung Injury (ALI)**. *Volume overloading of heart* - While fluid overload can cause pulmonary edema, the severity and rapid onset of distress after transfusion, coupled with the bilateral infiltrates, point more specifically to TRALI rather than isolated volume overload, especially in the context of FFP. - Cardiogenic pulmonary edema typically presents with **cardiomegaly** and signs of **heart failure**, which are not explicitly described or obviously seen as the primary cause in the given scenario and image. *Mendelson's syndrome* - Mendelson's syndrome, or **aspiration pneumonitis**, results from the inhalation of acidic gastric contents, leading to chemical pneumonitis. - This typically occurs in patients with impaired consciousness or those undergoing procedures that compromise airway protection, and there is no information in the vignette to suggest aspiration. *Pneumomediastinum* - Pneumomediastinum indicates the presence of **air in the mediastinum**, which would appear as radiolucent streaks outlining mediastinal structures on a CXR. - The image primarily shows diffuse bilateral infiltrates and pulmonary edema, rather than free air in the mediastinum.
Question 6: Identify the congenital heart disease presenting with cyanosis in CXR: (Recent NEET Pattern 2016-17)
- A. Tetralogy of Fallot (Correct Answer)
- B. Truncus Arteriosus
- C. Ebstein anomaly
- D. Snowman heart
Explanation: ***Tetralogy of Fallot*** - The chest X-ray shows a **boot-shaped heart** (coeur en sabot) due to right ventricular hypertrophy and a concave pulmonary artery segment, which is a classic finding in Tetralogy of Fallot. - This cyanotic congenital heart disease is characterized by four defects: a **ventricular septal defect**, **pulmonary stenosis**, **overriding aorta**, and **right ventricular hypertrophy**. *Truncus Arteriosus* - This cyanotic CHD involves a **single arterial trunk** arising from the heart supplying systemic, pulmonary, and coronary circulations. - CXR typically shows **cardiomegaly with increased pulmonary vascular markings** and a **right-sided aortic arch** in 30% of cases, not the boot-shaped heart seen here. - The pulmonary artery segment is **prominent or convex**, contrasting with the concave segment in Tetralogy of Fallot. *Ebstein anomaly* - This anomaly involves the **tricuspid valve** being displaced into the right ventricle, often leading to cardiomegaly and a **"box-shaped" or "globular" heart** on CXR, which is not depicted. - It can cause cyanosis, but the characteristic CXR finding is **massive cardiomegaly with diminished pulmonary vascular markings**, not a boot-shaped heart. *Snowman heart* - The "snowman heart" or **"figure of 8" sign** is characteristic of **total anomalous pulmonary venous return (TAPVR)**, specifically the supracardiac type. - This appearance is due to the dilated superior vena cava and the vertical vein draining into it, creating the "head" of the snowman, which is not seen in the provided image.
Question 7: A breast cancer patient presents with difficulty in breathing. CXR shows:
- A. Pneumothorax
- B. Pulmonary artery hypertension
- C. Interstitial lung disease
- D. Cannonball metastasis (Correct Answer)
Explanation: ***Cannonball metastasis*** - The chest X-ray shows multiple, well-defined, rounded opacities of varying sizes scattered throughout both lung fields, consistent with the characteristic appearance of **cannonball metastases**. - Given the patient's history of **breast cancer** and new onset **dyspnea**, pulmonary metastases are a very likely cause. *Pneumothorax* - A pneumothorax would appear as an area of translucency with absence of lung markings, often accompanied by a visible visceral pleural line and tracheal deviation in severe cases. This is not observed here; instead, the lungs are filled with multiple lesions. - The image does not show any signs of a collapsed lung, air in the pleural space, or shifted mediastinum. *Pulmonary artery hypertension* - Pulmonary artery hypertension on CXR might show **enlarged central pulmonary arteries** and pruning of peripheral vessels, or signs of right heart enlargement. - The predominant features in this image are numerous discrete nodules, not signs of vascular dilation or heart changes. *Interstitial lung disease* - Interstitial lung disease typically presents with a **reticular, nodular, or reticulonodular pattern**, often with reduced lung volumes and honeycombing in advanced stages. - The distinct, large, spherical lesions seen here are not characteristic of the diffuse, fine patterns associated with most interstitial lung diseases.
Question 8: An AIDS patient presents with respiratory distress. CXR shows:
- A. Pneumocystis pneumonia (Correct Answer)
- B. Miliary TB
- C. Streptococcal pneumonia
- D. Lymphocytic interstitial Pneumonitis
Explanation: ***Pneumocystis pneumonia*** - The chest X-ray shows **diffuse bilateral interstitial infiltrates**, which is a classic presentation of *Pneumocystis jirovecii pneumonia (PJP)* in an AIDS patient. - PJP is an **opportunistic infection commonly seen in immunocompromised individuals**, especially those with AIDS and low CD4 counts, presenting with respiratory distress. *Miliary TB* - Miliary TB would typically show **numerous small (1-3 mm), well-defined, uniformly distributed nodular opacities**, resembling millet seeds, which are not clearly visible here. - While TB is common in AIDS, the diffuse interstitial pattern is less characteristic of miliary spread. *Streptococcal pneumonia* - *Streptococcal pneumonia* often presents as **lobar consolidation with air bronchograms**, typically affecting one or more lobes, rather than the diffuse interstitial pattern seen in the image. - While it can occur in AIDS patients, the radiographic features are not consistent with this diagnosis. *Lymphocytic interstitial Pneumonitis* - *Lymphocytic interstitial pneumonitis (LIP)* is more common in **pediatric AIDS patients** and often presents with more pronounced **nodular or cystic changes** and interstitial infiltrates, but the primary pattern for this acute presentation of respiratory distress as seen would be PJP. - While it is a differential consideration in AIDS patients with interstitial lung disease, the abrupt onset of respiratory distress with diffuse infiltrates points more strongly to an acute infection.
Question 9: An 18-year-old boy is brought to the hospital with difficulty in breathing after a bar fight. What does the given CT chest show?
- A. Pneumothorax (Correct Answer)
- B. Consolidation
- C. Pulmonary contusion
- D. Haemothorax
Explanation: ***Pneumothorax*** - The CT image shows a clear **absence of lung parenchyma** extending to the chest wall, with a visible **visceral pleural line** separated from the parietal pleura. This indicates air in the pleural space, which is characteristic of a pneumothorax. - The patient presenting with **difficulty in breathing** after a bar fight (implying trauma) is consistent with a **traumatic pneumothorax**. *Consolidation* - **Consolidation** appears as a region of increased attenuation (whitening) on CT, usually with **air bronchograms**, indicating filling of alveolar spaces, which is not seen here. - While it can cause difficulty breathing, it results from infection or inflammation, not typically direct trauma creating an empty space like in the image. *Pulmonary contusion* - **Pulmonary contusion** would appear as areas of **ground-glass opacity** or **consolidation** within the lung parenchyma due to bleeding and edema, without a significant collapse of the lung. - The image distinctly shows a collapsed lung with a clear air-filled pleural space, not parenchymal injury. *Haemothorax* - A **hemothorax** would show a **fluid collection** (appearing white or grey) in the pleural space, often layering dependently, which is not the primary finding on this image where an air-filled space is prominent. - While a traumatic event could lead to both pneumothorax and hemothorax (**hemopneumothorax**), the most striking feature evident here is the air within the pleural cavity causing lung collapse.
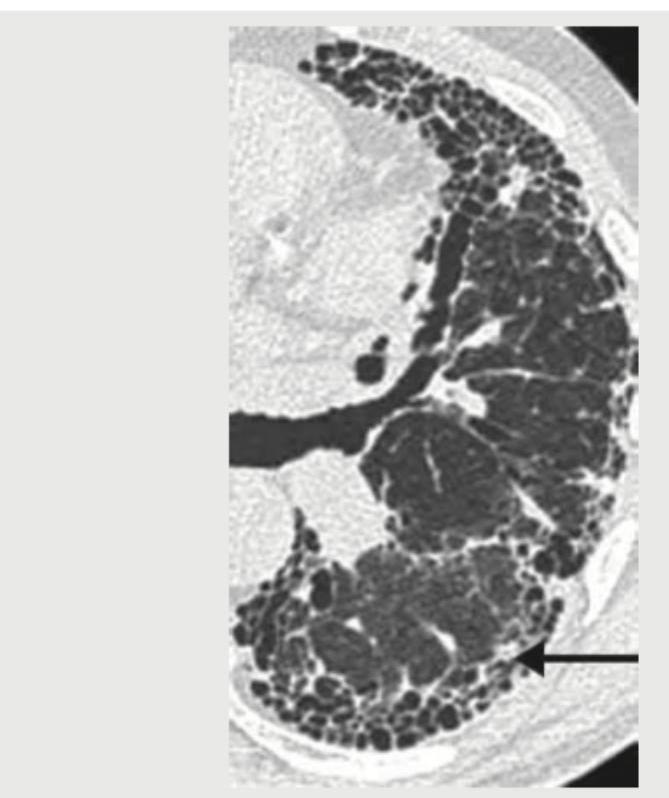
Question 10: The lung parenchyma on CT chest shown below is best described as:
- A. Honey comb pattern
- B. Signet ring pattern
- C. Crazy pavement pattern (Correct Answer)
- D. Mosaic pattern
Explanation: ***Crazy pavement pattern*** - The image distinctly shows a combination of **ground-glass opacities** and superimposed **interlobular septal thickening**, which together create the characteristic "crazy paving" appearance. - This pattern is most commonly associated with **pulmonary alveolar proteinosis**, but can also be seen in conditions like ARDS, PCP pneumonia, and lipoid pneumonia. *Honey comb pattern* - This pattern involves the presence of multiple, clustered, thick-walled **cysts** of varying sizes, typically subpleural, which are a sign of **end-stage lung fibrosis**. - While there are cystic changes in the image, the predominant finding includes ground-glass opacities and septal thickening rather than pure end-stage fibrotic changes. *Signet ring pattern* - A signet ring pattern is classically seen in **bronchiectasis**, where a dilated bronchus is paired with its accompanying smaller pulmonary artery, resembling a signet ring. - The image does not show clearly dilated bronchi adjacent to pulmonary arteries; instead, it displays diffuse parenchymal changes. *Mosaic pattern* - The mosaic pattern refers to areas of differing lung attenuation, often due to **air trapping** (causing dark areas) or areas of **perfusion abnormalities** (creating lighter areas), common in conditions like small airway disease or chronic thromboembolic disease. - While there is some heterogeneity, the specific combination of ground-glass and septal thickening is more accurately described as crazy paving.