NEET-PG 2017 — Pharmacology
8 Previous Year Questions with Answers & Explanations
A 50-year-old woman with rheumatic heart disease is on medication for heart disease. She feels unwell for most part of the day. Which of the following medicine is responsible for the ECG changes shown below? (Recent NEET Pattern 2016-17)
A 65-year-old patient of dilated cardiomyopathy was prescribed 1 mg warfarin tablet for sustained atrial fibrillation. The chemist however gave him 2 mg tablets by mistake which resulted in him developing hemorrhagic complications (bleeding). CT scan is performed. This is which kind of ADR? (Recent NEET Pattern 2016-17) Warfarin Sodium Tablets, USP Crystalline 2 mg Protect from light
The effect of both drugs given together on the blood pressure of a patient was evaluated in comparison with the effect of individual drugs on BP. The following curve represents: (Recent NEET Pattern 2016-17)
Drug A is epinephrine and drug B is cocaine. The effect of both drugs given together on the blood pressure of a patient was evaluated in comparison with effect of individual drugs on BP. The following curve represents:
A 20-year-old woman is admitted with the following presentation. 1% pilocarpine is not showing any response on the side of mydriasis. What is the diagnosis? (Recent NEET Pattern 2016-17)
A neonate presents with a congenital heart disease as shown below. Which drug should be started immediately? (Recent NEET Pattern 2016-17)
Which anti-epileptic drug marked X will act at the site shown?
The application of the following product can lead to development of: (Recent NEET Pattern 2016-17)
NEET-PG 2017 - Pharmacology NEET-PG Practice Questions and MCQs
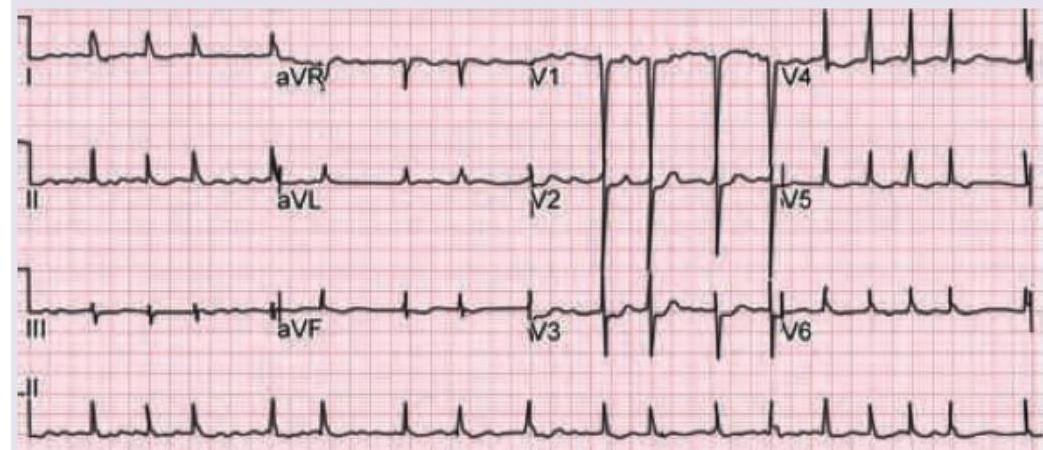
Question 1: A 50-year-old woman with rheumatic heart disease is on medication for heart disease. She feels unwell for most part of the day. Which of the following medicine is responsible for the ECG changes shown below? (Recent NEET Pattern 2016-17)
- A. ACE inhibitor
- B. Diuretics
- C. Ivabradine
- D. Digoxin (Correct Answer)
Explanation: ***Digoxin*** - The ECG shows changes characteristic of **digoxin toxicity**, specifically **downsloping ST depressions (scooping)** and **flattened or inverted T waves**, particularly in leads with dominant R waves. - The patient's symptoms of feeling "unwell for most part of the day" are consistent with **digoxin toxicity**, which can include nausea, fatigue, and cardiac arrhythmias. *ACE inhibitor* - ACE inhibitors primarily affect the **renin-angiotensin-aldosterone system** and do not typically cause these specific ECG changes. - Common side effects include cough and **hyperkalemia**, not the "scooped" ST segments seen here. *Diuretics* - Diuretics can cause **electrolyte imbalances**, such as hypokalemia, which might manifest as **flattened T waves** or **prominent U waves** on ECG, but not the characteristic "scooped" ST depression. - The symptoms of malaise are non-specific and while possible with electrolyte disturbances, the specific ECG pattern points away from diuretics as the primary cause. *Ivabradine* - Ivabradine is a **selective If channel inhibitor** that primarily reduces heart rate, without affecting myocardial contractility or repolarization significantly. - It does not cause the **ST segment changes** characteristic of digoxin effect or toxicity.
Question 2: A 65-year-old patient of dilated cardiomyopathy was prescribed 1 mg warfarin tablet for sustained atrial fibrillation. The chemist however gave him 2 mg tablets by mistake which resulted in him developing hemorrhagic complications (bleeding). CT scan is performed. This is which kind of ADR? (Recent NEET Pattern 2016-17) Warfarin Sodium Tablets, USP Crystalline 2 mg Protect from light
- A. Type A (Correct Answer)
- B. Type B
- C. Type C
- D. Type D
Explanation: ***Type A*** - This is an **exaggerated pharmacological effect** of warfarin due to a higher than intended dose, leading to excessive anticoagulation and subsequent **hemorrhagic stroke** (bleeding in the brain). - Type A ADRs are **predictable** based on the known pharmacology of the drug and are dose-dependent. *Type B* - Type B ADRs are **unpredictable**, idiosyncratic reactions that are not directly related to the pharmacological action of the drug (e.g., allergic reactions). - They are typically **dose-independent** and often occur in a small subset of the population. *Type C* - Type C ADRs are associated with **long-term exposure** to a drug, leading to chronic effects or tolerance. - Examples include drug dependence or adrenal suppression from prolonged corticosteroid use. *Type D* - Type D ADRs are also related to **delayed effects** of drug exposure, such as carcinogenesis or teratogenesis. - These effects may not manifest until months or years after the drug was taken.
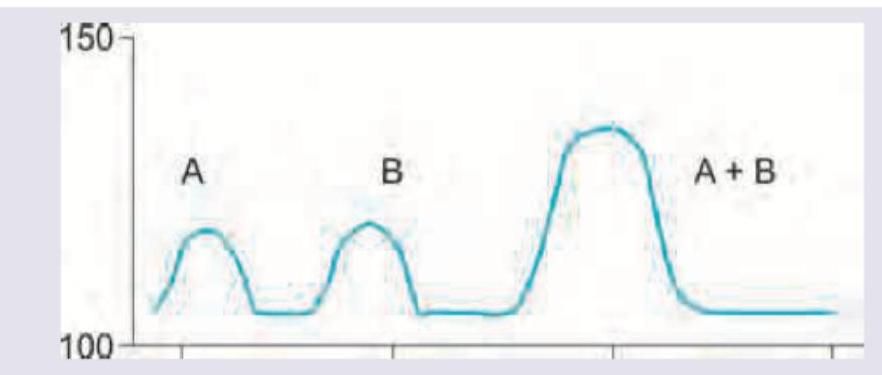
Question 3: The effect of both drugs given together on the blood pressure of a patient was evaluated in comparison with the effect of individual drugs on BP. The following curve represents: (Recent NEET Pattern 2016-17)
- A. Summation
- B. Additive effects
- C. Synergism (Correct Answer)
- D. Antagonism
Explanation: ***Synergism*** - The graph shows that the effect of drugs A and B when given together (A+B) is significantly **greater than the sum of their individual effects**. - This amplified effect, where the combined response is more than the simple addition of individual responses, is the definition of **synergism** (also called potentiation or supra-additive effect). *Summation* - Summation occurs when the **combined effect** of two drugs is **equal to the arithmetic sum** of their individual effects. - In the depicted graph, the peak effect of A+B is clearly much higher than the sum of the peaks of A and B individually, ruling out simple summation. *Additive effects* - Additive effects are synonymous with summation, meaning the combined effect is precisely the sum of individual effects. - The graph demonstrates a response that **exceeds a simple additive effect**, indicating a synergistic interaction rather than mere additive action. *Antagonism* - **Antagonism** occurs when one drug reduces or blocks the effect of another drug, resulting in a combined effect that is **less than the sum** of individual effects. - In the depicted graph, the combined effect (A+B) clearly shows enhancement rather than reduction, ruling out antagonism.
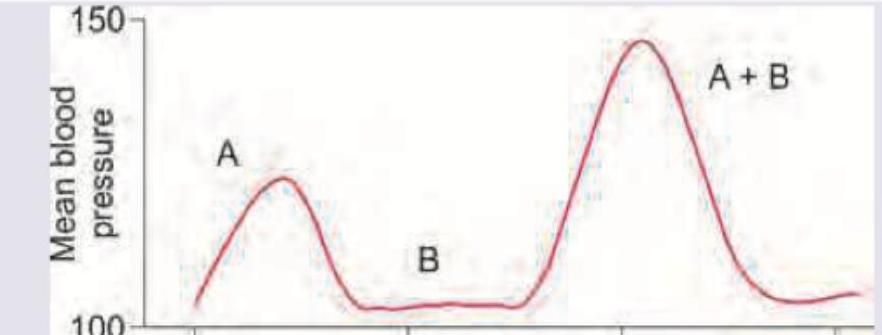
Question 4: Drug A is epinephrine and drug B is cocaine. The effect of both drugs given together on the blood pressure of a patient was evaluated in comparison with effect of individual drugs on BP. The following curve represents:
- A. Summation
- B. Additive effects
- C. Synergism (Correct Answer)
- D. Antagonism
Explanation: ***Synergism*** - **Synergism** occurs when the combined effect of two drugs is significantly greater than the sum of their individual effects. In the provided graph, the peak blood pressure with drugs A+B is notably higher than the sum of the peaks for A and B administered separately. - Epinephrine (Drug A) is a **vasoconstrictor**, and cocaine (Drug B) **inhibits norepinephrine reuptake**, potentiating epinephrine's effects by increasing synaptic levels of catecholamines. This leads to a much stronger combined increase in blood pressure than expected from simple addition. *Summation* - **Summation** implies that the combined effect of two drugs is equal to the sum of their individual effects. - The graph clearly shows that the combined effect (A+B) produces a blood pressure response that is much greater than simply adding the individual responses of A and B, ruling out summation. *Additive effects* - **Additive effects** are a type of summation where the combined effect of two or more drugs is numerically equal to the arithmetic sum of their individual effects. - Similar to summation, this option is incorrect because the observed combined effect of A and B is significantly *more* than the mathematical sum of their separate effects, indicating potentiation rather than simple additivity. *Antagonism* - **Antagonism** occurs when one drug reduces or blocks the effect of another drug. - This is incorrect because the graph shows that the combined administration of epinephrine and cocaine produces a *greater* blood pressure response, not a reduced one. Antagonism would result in a combined effect less than expected or less than either drug alone.
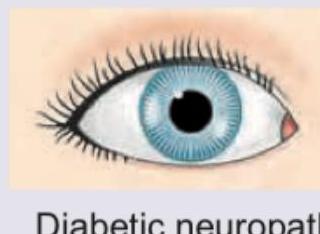
Question 5: A 20-year-old woman is admitted with the following presentation. 1% pilocarpine is not showing any response on the side of mydriasis. What is the diagnosis? (Recent NEET Pattern 2016-17)
- A. Pharmacological block (Correct Answer)
- B. Diabetic neuropathy
- C. Uncal herniation
- D. Adie tonic pupil
Explanation: ***Pharmacological block*** - A **dilated pupil** that shows **no response to 1% pilocarpine** is characteristic of **pharmacological mydriasis** caused by anticholinergic agents (atropine, scopolamine, tropicamide, homatropine). - The muscarinic receptors on the iris sphincter muscle are **competitively blocked** by these agents, preventing acetylcholine and even exogenous pilocarpine from causing pupillary constriction. - This is the **key distinguishing feature** from other causes of mydriasis: the pupil remains dilated despite administration of cholinergic agonists. - Common scenarios include **accidental exposure** to belladonna alkaloids, intentional cosmetic use, or contamination from medications. *Adie tonic pupil* - Adie's tonic pupil presents with a **dilated pupil with sluggish or absent light reflex**, but it shows **positive response to dilute pilocarpine (0.125%)** due to **denervation supersensitivity**. - This supersensitivity is the hallmark diagnostic feature distinguishing Adie's from other causes. - Since this patient shows **no response to 1% pilocarpine** (a much higher concentration), Adie's pupil is ruled out. - Typically seen in young women with **vermicular iris movements** on slit-lamp examination. *Diabetic neuropathy* - Diabetic autonomic neuropathy may affect pupillary responses, but typically causes **smaller pupils** with impaired dilation rather than fixed mydriasis. - Would be associated with other signs of diabetic neuropathy: **peripheral neuropathy, gastroparesis, orthostatic hypotension**. - Does not present as isolated, fixed mydriasis unresponsive to pilocarpine. *Uncal herniation* - Results from **compression of CN III (oculomotor nerve)** due to increased intracranial pressure. - Causes a **"blown pupil"** (dilated and fixed) with associated **ptosis and eye positioned "down and out"**. - This is a **neurosurgical emergency** with altered consciousness, not consistent with a stable outpatient presentation in a young woman. - The pupil may show minimal response to strong pilocarpine, but the clinical context is entirely different.
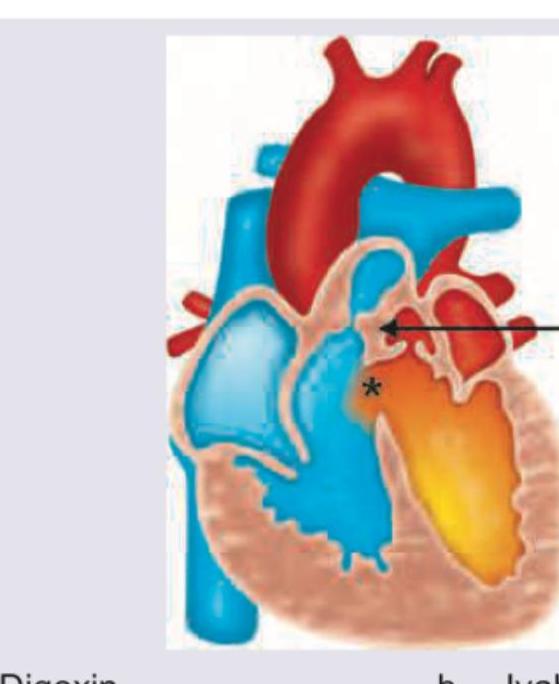
Question 6: A neonate presents with a congenital heart disease as shown below. Which drug should be started immediately? (Recent NEET Pattern 2016-17)
- A. Digoxin
- B. Ivabradine
- C. Propranolol
- D. Alprostadil (Correct Answer)
Explanation: ***Alprostadil*** - The image shows a **transposition of the great arteries (TGA)** with the aorta originating from the right ventricle and the pulmonary artery from the left ventricle. In this condition, a patent ductus arteriosus (PDA) is crucial to maintain mixing of oxygenated and deoxygenated blood to ensure systemic circulation. - **Alprostadil (prostaglandin E1 analog)** is used to keep the **ductus arteriosus patent**, allowing for mixing of blood and improving systemic oxygenation in neonates with ductal-dependent congenital heart defects like severe TGA. *Digoxin* - **Digoxin** is a cardiac glycoside used to improve **cardiac contractility** and control heart rate in certain heart conditions, but it is not the immediate drug of choice for maintaining patency of the ductus arteriosus in TGA. - Its primary role is in managing heart failure symptoms or arrhythmias, not directly addressing the immediate ductal dependency of TGA. *Ivabradine* - **Ivabradine** is a hyperpolarization-activated cyclic nucleotide-gated (HCN) channel blocker that selectively reduces heart rate by acting on the **sinoatrial node**. - It is used in adults with chronic heart failure or stable angina, and is not indicated for the acute management of congenital heart defects like TGA in neonates. *Propranolol* - **Propranolol** is a non-selective beta-blocker used to reduce heart rate and blood pressure, or to manage conditions like **tetralogy of Fallot spells**. - It does not have any role in maintaining the patency of the ductus arteriosus, which is critical for survival in ductal-dependent congenital heart lesions like TGA.
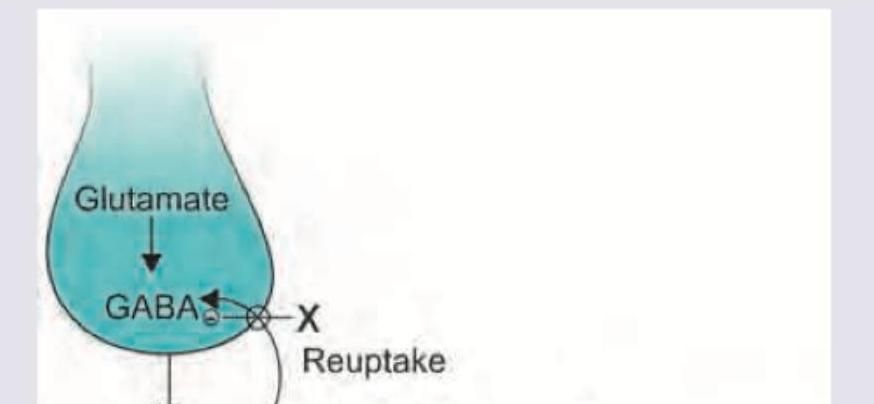
Question 7: Which anti-epileptic drug marked X will act at the site shown?
- A. Tiagabine (Correct Answer)
- B. Vigabatrin
- C. Gabapentin
- D. Rufinamide
Explanation: ***Tiagabine*** - The image shows site 'X' as a **GABA reuptake transporter** that actively removes GABA from the synaptic cleft back into the presynaptic neuron or glial cells - **Tiagabine** specifically inhibits **GABA reuptake transporters (GAT-1)**, thereby increasing GABA concentration in the synaptic cleft and enhancing its inhibitory effect - This is the mechanism directly targeting the site shown in the diagram *Vigabatrin* - Irreversible inhibitor of **GABA transaminase (GABA-T)**, the enzyme responsible for catabolizing GABA - Acts intracellularly to prevent GABA breakdown, not at the synaptic reuptake transporter shown - Different mechanism from the site depicted *Gabapentin* - GABA analog but does not bind to GABA receptors or interfere with GABA reuptake - Primary mechanism involves modulating **voltage-gated calcium channels (α2δ subunit)**, reducing excitatory neurotransmitter release - Does not act at GABA transporters *Rufinamide* - Prolongs the inactive state of **voltage-dependent sodium channels**, reducing neuronal excitability - Mechanism is distinct from GABA reuptake or metabolism - Does not act at the site shown in the diagram
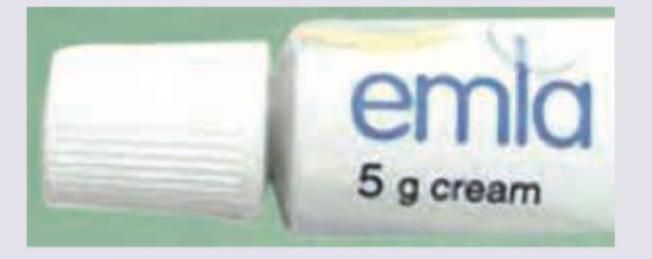
Question 8: The application of the following product can lead to development of: (Recent NEET Pattern 2016-17)
- A. Seizures
- B. Methemoglobinemia (Correct Answer)
- C. Depression
- D. Hypertension
Explanation: ***Methemoglobinemia (Correct)*** - EMLA cream contains **lidocaine** and **prilocaine**, both of which are **amide-type local anesthetics** - Prilocaine, in particular, can cause methemoglobinemia due to its metabolite, **o-toluidine**, which oxidizes hemoglobin to methemoglobin - While methemoglobinemia is rare with proper use, it is a known and serious adverse effect, especially when applied to large areas, on broken skin, or in infants - This is the most specific adverse effect associated with prilocaine in EMLA cream *Seizures (Incorrect)* - Seizures are a known systemic toxicity of local anesthetics like lidocaine and prilocaine but are usually associated with **very high systemic concentrations**, often from accidental intravenous injection or excessive application over large areas - While possible with overdose, methemoglobinemia is a more specific and direct concern linked to prilocaine's metabolic pathway - CNS toxicity typically requires systemic absorption beyond what occurs with proper topical use *Depression (Incorrect)* - Depression is **not a direct or common adverse effect** of EMLA cream or its components - Systemic absorption of local anesthetics can cause central nervous system effects, but depression is generally not among them - CNS effects more commonly involve excitation (restlessness, tremors) or sedation depending on the dose *Hypertension (Incorrect)* - Local anesthetics generally cause **vasodilation** at therapeutic doses, potentially leading to **hypotension** rather than hypertension, especially with systemic absorption - Hypertension is not a characteristic side effect associated with the topical application of EMLA cream - The cardiovascular effects of local anesthetics, when present, typically involve decreased blood pressure and myocardial depression