A 3-year-old girl brought with swelling in left eye which had shown rapid growth in last 4 weeks. On examination it is a bulbous fleshy mass about 5 x 4 cm arising from lower eyelid. No organomegaly or was noted and lymph node examination was unremarkable. The Complete blood counts are normal. Probable diagnosis is?
All are true about the child shown in the image except:
A 1-year-old unimmunised child with HbsAg positivity is having following skin lesions. What is the diagnosis?

A 5-year-old child in a village went for open air defecation when he was attacked by a dog. He has been admitted in your hospital, all are correct about the condition except: (Recent NEET Pattern 2016-17)

A 2-year-old unimmunized child from a village presents with fever, decreased feeding and ear ache. All are true about the virus responsible for the condition shown except: (Recent NEET Pattern 2016-17)

A child presents with the ocular findings shown in the image below. Identify the most likely underlying illness:
A 12-year-old boy presents with difficulty in reading from the blackboard in school. Initially refraction error was considered but visual acuity was normal. He has started complaining of diplopia on watching TV or after studying for long. He takes very long time to finish his meals and his speech becomes very difficult to understand after speaking continuously for few minutes. Anti-Acetylcholine receptor blocking antibody is detected in high titers. All are done in management except? (Recent NEET Pattern 2016-17)
The image shows:

NEET-PG 2017 - Pediatrics NEET-PG Practice Questions and MCQs
Question 21: A 3-year-old girl brought with swelling in left eye which had shown rapid growth in last 4 weeks. On examination it is a bulbous fleshy mass about 5 x 4 cm arising from lower eyelid. No organomegaly or was noted and lymph node examination was unremarkable. The Complete blood counts are normal. Probable diagnosis is?
- A. Retinoblastoma
- B. Rhabdomyosarcoma (Correct Answer)
- C. Chloroma
- D. Orbital metastasis
Explanation: ***Rhabdomyosarcoma*** - This is the most common **primary orbital malignancy in children**, often presenting as a rapidly growing, fleshy periorbital mass, consistent with the 3-year-old girl's symptoms. - The rapid growth (4 weeks) and the description of a **bulbous, fleshy mass** arising from the eyelid are classic presentations of rhabdomyosarcoma. *Retinoblastoma* - This is a malignancy of the retina and typically presents with **leukocoria (white pupillary reflex)**, strabismus, or vision impairment, not usually as an external fleshy mass arising from the eyelid. - While it is a common pediatric eye tumor, its clinical presentation differs significantly from the described external swelling. *Chloroma* - Also known as granulocytic sarcoma, chloroma is an extramedullary manifestation of **acute myeloid leukemia** and would typically be associated with systemic symptoms of leukemia (e.g., anemia, thrombocytopenia, leukocytosis/leukopenia) and abnormal blood counts. - The patient's normal CBC and lack of organomegaly/lymphadenopathy make chloroma less likely. *Orbital metastasis* - While possible, orbital metastases in children are rare and typically arise from **neuroblastoma** or occasionally other primary tumors. - Such metastases usually present with features suggestive of the primary tumor, which are not mentioned here.
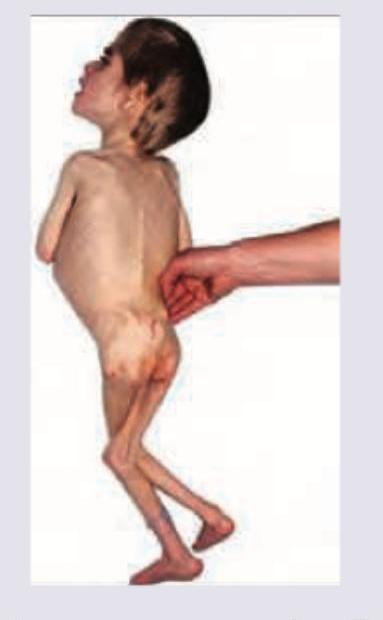
Question 22: All are true about the child shown in the image except:
- A. Baggy pants appearance
- B. Apathy
- C. Reduced MAC
- D. Delayed skin pinch (Correct Answer)
Explanation: ***Delayed skin pinch*** - Delayed skin pinch, also known as **poor skin turgor**, is a sign of **dehydration**, which is more characteristic of **kwashiorkor** or severe acute malnutrition with significant fluid loss, rather than marasmus alone. - In marasmus, although there is severe wasting, **skin turgor is often preserved** due to the absence of significant edema. - This is the **EXCEPTION** - it is NOT a typical feature of pure marasmus. *Baggy pants appearance* - The **extreme loss of subcutaneous fat and muscle mass** in marasmus causes the skin around the buttocks and thighs to hang loosely, creating a "baggy pants" or "old man" appearance. - This is a **hallmark feature** indicating severe wasting in marasmus. *Apathy* - Children with severe marasmus often exhibit **apathy, irritability, and decreased activity**, reflecting their profound energy deficit and associated psychological distress. - This is a common neurological and behavioral manifestation of **severe malnutrition**. *Reduced MAC* - **Mid-upper arm circumference (MAC)** is severely reduced in marasmus due to the significant loss of both fat and muscle tissue in the upper arm. - A **MAC less than 11.5 cm** is a key diagnostic criterion for **severe acute malnutrition** in children aged 6-59 months.
Question 23: A 1-year-old unimmunised child with HbsAg positivity is having following skin lesions. What is the diagnosis?
- A. Gianotti-Crosti syndrome (Correct Answer)
- B. Erythema infectiosum
- C. Pityriasis alba
- D. Pityriasis rosea
Explanation: ***Gianotti-Crosti syndrome*** - This syndrome is characterized by a **papular acrodermatitis** of childhood, typically presenting as monomorphic, erythematous papules on the face, buttocks, and extensor surfaces of the extremities. - It is strongly associated with **viral infections**, particularly **Hepatitis B virus (HBV)** and Epstein-Barr virus (EBV), which aligns with the HbsAg positivity in this unimmunized child. *Erythema infectiosum* - This condition is caused by **Parvovirus B19** and typically presents with a "slapped cheek" rash on the face, followed by a lacy, reticulated rash on the trunk and extremities. - The rash in the image does not demonstrate the characteristic lacy pattern or typical "slapped cheek" appearance. *Pityriasis alba* - This is a common, mild, and often asymptomatic skin condition characterized by **hypopigmented (lighter) patches** with fine scales, predominantly on the face and arms. - The lesions in the image are erythematous (red) and papular, not hypopigmented. *Pityriasis rosea* - This condition typically begins with a single, larger "herald patch" followed by smaller, oval-shaped, pinkish-red patches with a characteristic **"Christmas tree" pattern** on the trunk and proximal extremities. - The rash in the image does not show a herald patch or the distinct distribution and morphology of pityriasis rosea.
Question 24: A 5-year-old child in a village went for open air defecation when he was attacked by a dog. He has been admitted in your hospital, all are correct about the condition except: (Recent NEET Pattern 2016-17)
- A. Category 3 bite
- B. Wash with povidone-iodine
- C. Administer vero cell vaccine with immunoglobulin
- D. Virus infects pyramidal cells leading to cytolysis (Correct Answer)
Explanation: ***Virus infects pyramidal cells leading to cytolysis*** - The **rabies virus** primarily infects neurons and causes neuronal dysfunction rather than **cytolysis** (cell death and lysis), particularly in the early stages. - The characteristic pathological finding in rabies is the presence of **Negri bodies** (intracytoplasmic inclusions) which represent viral aggregates within unaffected neurons, not cytolytic destruction. *Category 3 bite* - A **Category 3 bite** involves single or multiple transdermal bites or scratches, licks on broken skin, or contamination of mucous membranes with saliva, especially if involving the head, neck, or digits, which appears to be the case given the severe facial injuries depicted with a dog bite. - Due to the high risk of rabies transmission in such severe wounds, Category 3 requires both **rabies vaccine** and **rabies immunoglobulin (RIG)** administration. *Wash with povidone-iodine* - Immediate and thorough **wound washing** with soap and water for at least 15 minutes is crucial for all animal bites, as it significantly reduces the viral load. - **Antiseptics** like povidone-iodine or alcohol can be used after washing to further disinfect the wound. *Administer vero cell vaccine with immunoglobulin* - For a **Category 3 rabies exposure**, both **rabies vaccine** (e.g., Vero cell vaccine) and **rabies immunoglobulin (RIG)** are indicated for post-exposure prophylaxis. - The vaccine provides active immunity, while the immunoglobulin provides immediate passive immunity, critical for high-risk exposures.
Question 25: A 2-year-old unimmunized child from a village presents with fever, decreased feeding and ear ache. All are true about the virus responsible for the condition shown except: (Recent NEET Pattern 2016-17)
- A. Belongs to genus morbillivirus (Correct Answer)
- B. Nonsuppurative parotitis
- C. Can lead to aseptic meningitis
- D. Causative virus possesses both H and N proteins
Explanation: The image shows a child with characteristic swelling of the parotid gland, indicative of Mumps. The clinical presentation (unimmunized child, fever, decreased feeding, ear ache, and parotid swelling) strongly points to Mumps. ***Correct Answer: Belongs to genus morbillivirus*** - This statement is **FALSE** and therefore the correct answer to this "EXCEPT" question. - The virus responsible for Mumps is the **Mumps virus**, which belongs to the **genus Rubulavirus** within the family Paramyxoviridae, NOT Morbillivirus. - Morbillivirus is the genus to which the **Measles virus** belongs. *Incorrect: Nonsuppurative parotitis* - **TRUE statement** - Mumps is classically characterized by **nonsuppurative parotitis**, meaning inflammation of the salivary glands (primarily parotid) without pus formation. - This is a key diagnostic feature of Mumps. *Incorrect: Can lead to aseptic meningitis* - **TRUE statement** - Aseptic meningitis is one of the most common and significant complications of Mumps, occurring in 10-15% of cases. - This complication typically presents with headache, stiff neck, and photophobia, without bacterial infection. *Incorrect: Causative virus possesses both H and N proteins* - **TRUE statement** - The Mumps virus, a member of the Paramyxoviridae family, possesses a combined **HN (hemagglutinin-neuraminidase) protein** on its surface. - The HN protein has both hemagglutinin and neuraminidase activities, responsible for binding to host cells and facilitating release of new virions from infected cells.
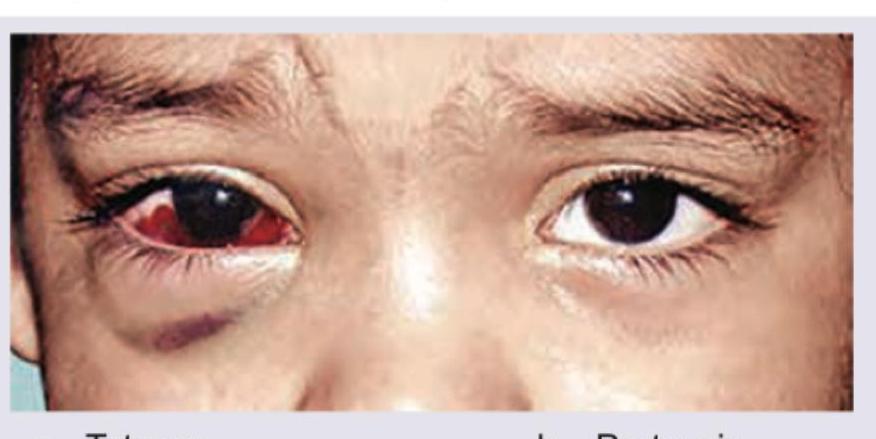
Question 26: A child presents with the ocular findings shown in the image below. Identify the most likely underlying illness:
- A. Tetanus
- B. Measles
- C. Trachoma
- D. Pertussis (Correct Answer)
Explanation: ***Pertussis (Whooping Cough)*** - The image shows **subconjunctival hemorrhage**, which is a **classic complication** of pertussis in children - Pertussis causes severe **paroxysmal coughing fits** that dramatically increase intrathoracic and intravascular pressure - This elevated pressure leads to rupture of conjunctival blood vessels, resulting in subconjunctival hemorrhages and facial petechiae - These hemorrhages are well-recognized **diagnostic clues** for pertussis, especially when accompanied by the characteristic whooping cough - This is a **primary manifestation** of the disease process, not merely an incidental finding *Trachoma* - Trachoma, caused by *Chlamydia trachomatis*, presents with **chronic follicular conjunctivitis** and progressive scarring - Classic features include follicles on upper tarsal conjunctiva, conjunctival scarring, trichiasis, and pannus formation - While it causes conjunctival inflammation, **acute subconjunctival hemorrhage is NOT a typical feature** of trachoma - Trachoma is a chronic, scarring disease rather than an acute hemorrhagic condition *Tetanus* - Tetanus is a neurological disorder characterized by **muscle rigidity** and **spasms**, beginning with trismus (lockjaw) - Ocular manifestations are limited to **risus sardonicus** (facial muscle spasm) and potential ophthalmoplegia - Does NOT cause subconjunctival hemorrhage as a direct manifestation *Measles* - Measles presents with **maculopapular rash**, fever, the three C's (cough, coryza, conjunctivitis), and **Koplik spots** - The conjunctivitis in measles is typically a **bilateral, non-hemorrhagic inflammation** with watery discharge - Does NOT typically cause prominent subconjunctival hemorrhage as shown in the image
Question 27: A 12-year-old boy presents with difficulty in reading from the blackboard in school. Initially refraction error was considered but visual acuity was normal. He has started complaining of diplopia on watching TV or after studying for long. He takes very long time to finish his meals and his speech becomes very difficult to understand after speaking continuously for few minutes. Anti-Acetylcholine receptor blocking antibody is detected in high titers. All are done in management except? (Recent NEET Pattern 2016-17)
- A. Pyridostigmine
- B. Atropine (Correct Answer)
- C. Steroids
- D. CT chest
Explanation: ***Atropine*** - The patient's symptoms (diplopia, dysphagia, dysarthria, and improvement with rest, along with high titers of **anti-acetylcholine receptor blocking antibody**) are classic for **myasthenia gravis (MG)** [1], [2]. - **Atropine** is an anticholinergic agent that may occasionally be used to manage muscarinic side effects of cholinesterase inhibitors (like pyridostigmine), such as bradycardia, hypersalivation, or diarrhea [3]. - However, **atropine is NOT a primary treatment modality for MG** and is not part of routine management protocols [3]. It does not address the underlying pathophysiology or improve muscle strength. - In contrast, the other options represent core components of MG management. *Pyridostigmine* - **Pyridostigmine** is an **acetylcholinesterase inhibitor** and is the **first-line symptomatic treatment** for myasthenia gravis [1]. - It increases the amount of acetylcholine available at the neuromuscular junction, improving muscle strength and function. *Steroids* - **Corticosteroids** (like prednisone) are a mainstay of **immunosuppressive therapy** for myasthenia gravis, used to reduce the autoimmune attack on acetylcholine receptors [1]. - They are typically used when symptoms are not adequately controlled by pyridostigmine alone or in moderate to severe cases. *CT chest* - A **CT scan of the chest** is crucial in the initial workup of myasthenia gravis to screen for a **thymoma**, a tumor of the thymus gland. - Thymomas are associated with MG in 10-15% of patients, and their presence often dictates the need for thymectomy. - Even in the absence of thymoma, thymic hyperplasia is common in MG patients.
Question 28: The image shows:
- A. Defense wounds
- B. Hesitation cuts (Correct Answer)
- C. Radiation injury
- D. Homicidal stab
Explanation: ***Hesitation cuts*** - The image displays multiple, superficial, parallel incised wounds, primarily on the wrist, which are classic characteristics of **hesitation cuts**. - These wounds are often made by individuals contemplating **suicide** and are typically not immediately life-threatening, reflecting a tentative or experimental attempt before a deeper, fatal cut. *Defense wounds* - **Defense wounds** typically appear on the hands, forearms, and sometimes the legs, resulting from an individual instinctively shielding themselves from an assault. - They tend to be more varied in depth and pattern, often showing signs of struggle and resistance, unlike the uniform, superficial nature seen here. *Radiation injury* - **Radiation injury** or radiation dermatitis presents with skin changes ranging from erythema, desquamation, blistering, or hyperpigmentation, depending on the dose and duration of exposure. - These injuries do not typically involve sharp, incised wounds like those depicted in the image. *Homicidal stab* - A **homicidal stab** implies a deep, forceful wound intended to cause death, often characterized by a single or few much deeper penetrating wounds. - The superficial and numerous nature of the cuts in the image is inconsistent with the typical presentation of a homicidal attack.