All SubjectsAnatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (16)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q11
A neonate presents with the clinical features shown in the image below. What is the most likely diagnosis?
Q12
A newborn presents with macrosomia, plethoric appearance, and generalized edema. The image shows:

Q13
A 2-day-old neonate under phototherapy unit. For exchange transfusion serum bilirubin-albumin ratio should be: (Recent NEET Pattern 2016-17)
Q14
All are true about the swelling on scalp of a 2-day old neonate except: (Recent NEET Pattern 2016-17)
Q15
Which of the following interventions is being done in this neonate?

Q16
A 3-year-old child presents with sudden onset generalized petechiae and bruise on forehead. Sternal tenderness is absent and liver and spleen are not palpable. Bone marrow aspiration is normal. Probable cause is? (Recent NEET Pattern 2016-17)
Q17
A 6-month-old child brought by parents for diffuse ecchymosis on extremities and trunk. Probable diagnosis is? (Recent NEET Pattern 2016-17)

Q18
A 6-month-old infant with a progressively increasing abdominal lump. Investigations revealed a stage IVs neuroblastoma. All are correct about the condition except:
Q19
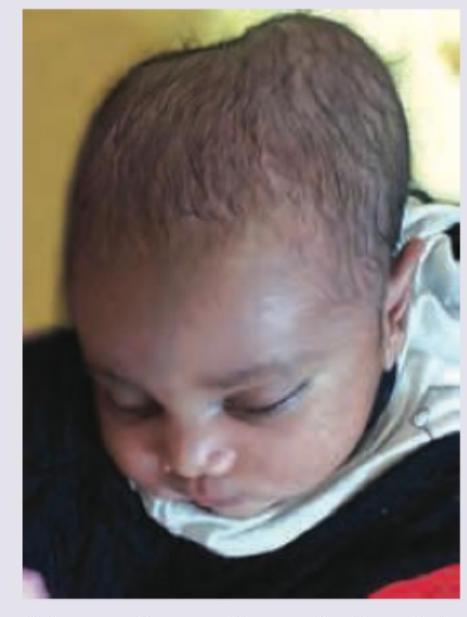
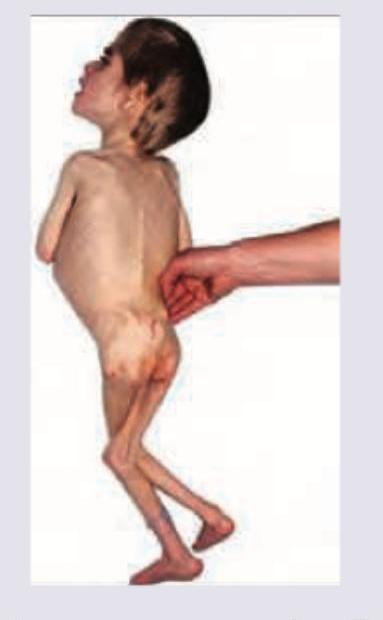
All are true about the child shown in the image except:
Q20
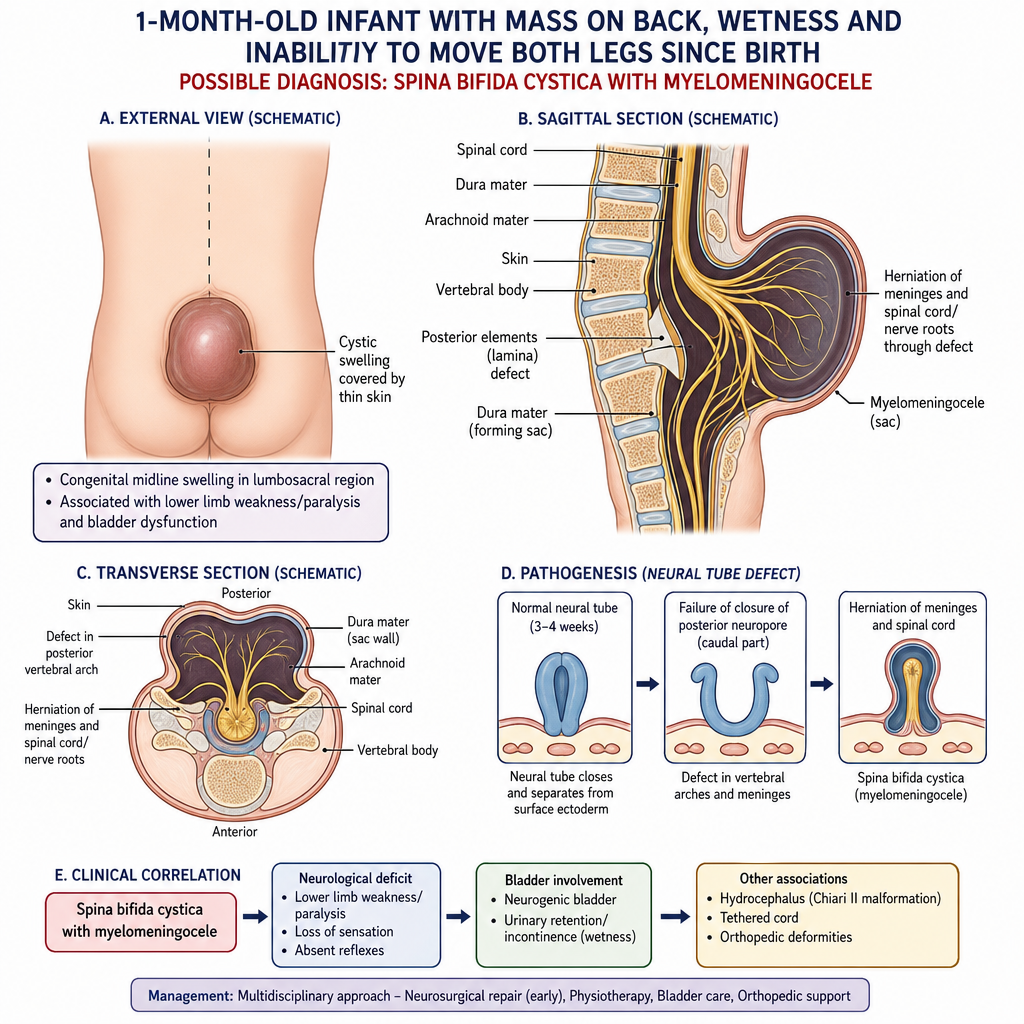
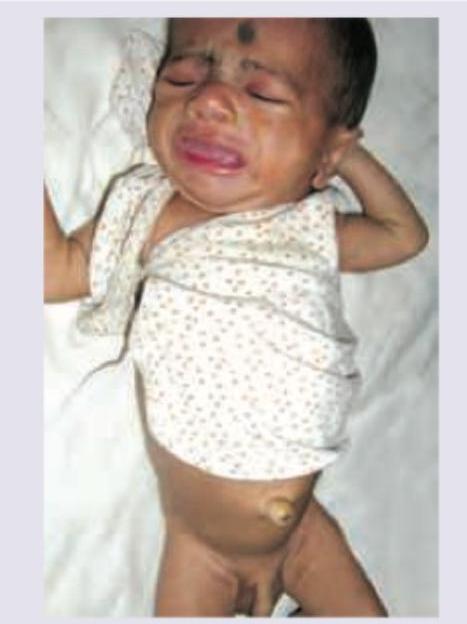
A 1-month-old baby brought by the mother complaining of a mass on back associated with wetness and inability of both legs to move ever since birth. Possible diagnosis: (Recent NEET Pattern 2016-17)