NEET-PG 2017 — Pediatrics
28 Previous Year Questions with Answers & Explanations
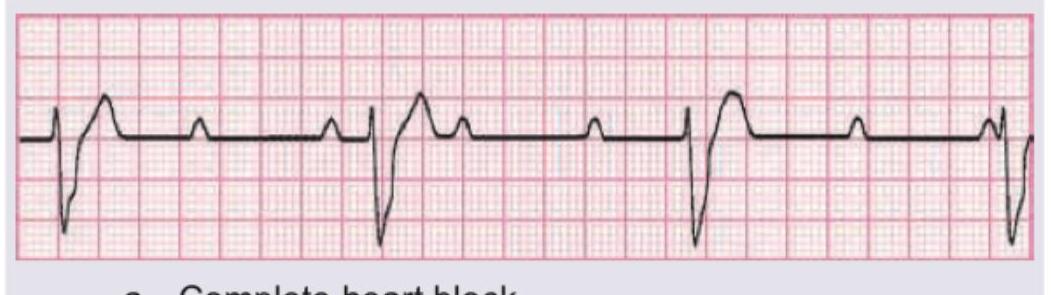
The given ECG of a neonate born to a mother with SLE shows?
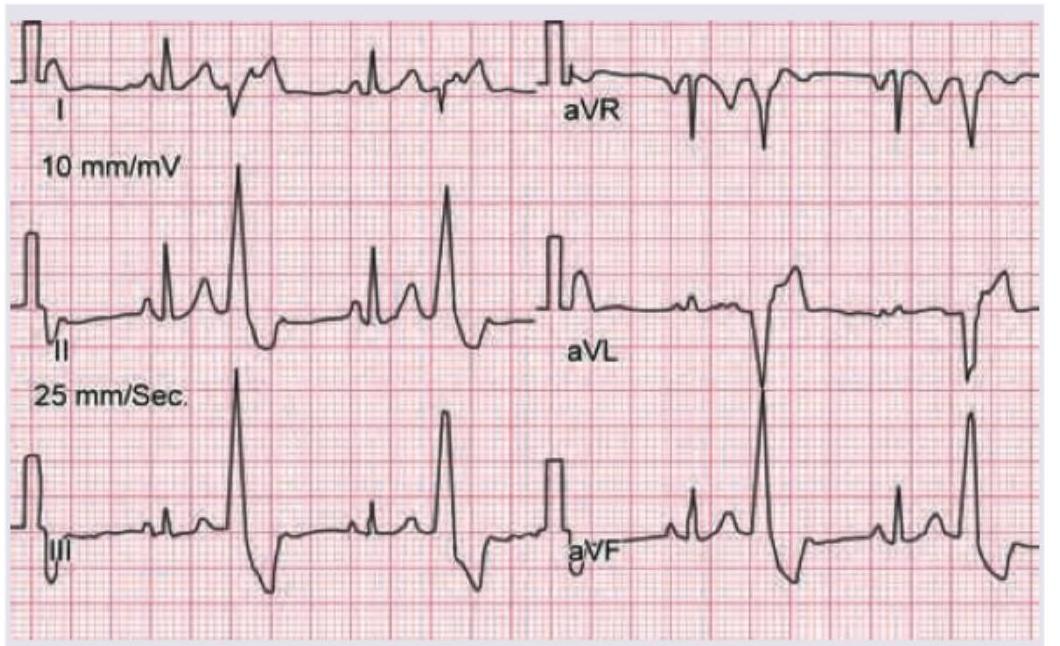
A 10-year-old child with Valvular heart disease on heart failure treatment, has the following ECG tracing. What is the diagnosis?
A 3-year-old child presents with the clinical features shown in the image. What is the most likely diagnosis?

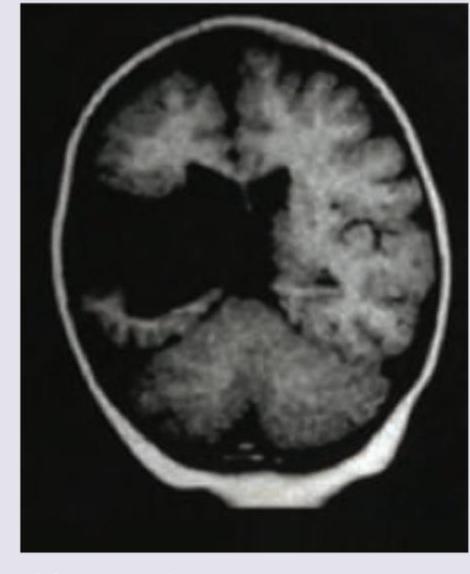
A 2-year-old epileptic child with developmental delay presents to emergency with fever for the last two days. NCCT shows:
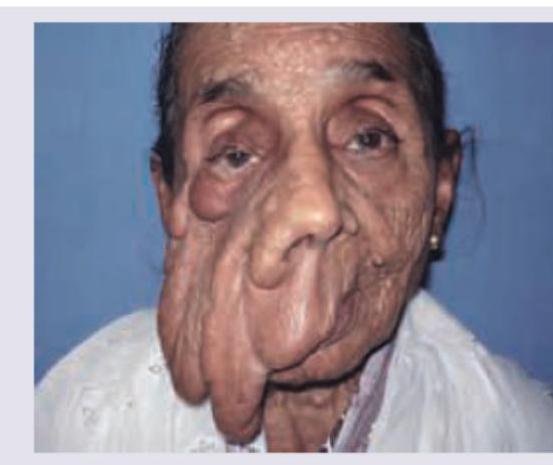
Comment on the diagnosis based on the image shown below. (Recent NEET Pattern 2016-17)
Which of the following is correct about the image shown? (Recent NEET Pattern 2016-17)
Comment on the diagnosis of this child, presenting with eye swelling. (Recent NEET Pattern 2016-17)
Neonate born at 34 weeks with premature rupture of membranes develops respiratory distress. CXR was performed. All are considered in differential diagnosis except:
Preterm child on cow milk due to death of mother is having blood in stools. X-ray abdomen was done. Diagnosis is:

Which of the following is the best diagnosis of this neonate who is excessively hungry, warm with flushed skin?
NEET-PG 2017 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: The given ECG of a neonate born to a mother with SLE shows?
- A. Complete heart block (Correct Answer)
- B. Mobitz I heart block
- C. Mobitz II heart block
- D. Sick sinus syndrome
Explanation: ***Complete heart block*** - The ECG demonstrates **complete dissociation** between the P waves (atrial activity) and the QRS complexes (ventricular activity). The atrial rate is faster than the ventricular rate, and there is no consistent relationship between P waves and QRS complexes. - In a neonate of a mother with SLE, **congenital complete heart block** is a well-known complication due to transplacental transfer of maternal antibodies (anti-Ro/SSA and anti-La/SSB) that damage the atrioventricular (AV) node. *Mobitz I heart block* - This type of heart block (also known as **Wenckebach phenomenon**) is characterized by a **progressive prolongation of the PR interval** until a P wave is eventually not conducted, leading to a dropped QRS complex. - The ECG provided does not show a gradual lengthening of the PR interval; rather, it shows a complete lack of conduction between atria and ventricles. *Mobitz II heart block* - In Mobitz II block, there is a **fixed PR interval** for conducted beats, but some P waves are **intermittently blocked** without prior PR prolongation. - The ECG in the question shows no consistent PR interval whatsoever, as P waves and QRS complexes are completely dissociated. *Sick sinus syndrome* - This condition involves a malfunction of the **sinoatrial node**, leading to a variety of rhythm disturbances such as sinus bradycardia, sinus arrest, or *tachycardia-bradycardia syndrome*. - While it can cause bradycardia, it does not typically present with the **P-QRS dissociation** characteristic of advanced AV block seen in the ECG.
Question 2: A 10-year-old child with Valvular heart disease on heart failure treatment, has the following ECG tracing. What is the diagnosis?
- A. Tall tented T-wave
- B. Ventricular bigeminy
- C. Non paroxysmal atrial tachycardia with irregular AV block
- D. Non paroxysmal atrial tachycardia with regular AV block (Correct Answer)
Explanation: ***Non paroxysmal atrial tachycardia with regular AV block*** - The ECG shows a sustained atrial tachycardia with a **consistent P-P interval**, indicating a non-paroxysmal origin. - There is a **fixed ratio between P waves and QRS complexes** (e.g., 2:1 or 3:1), demonstrating a regular AV block, likely due to increased vagal tone or AV nodal dysfunction, often seen in cases of **digoxin toxicity** (given the patient is on heart failure treatment for valvular heart disease). *Tall tented T-wave* - **Tall, tented T-waves** are characteristic of **hyperkalemia**, but the ECG tracing does not exhibit this morphology. - While hyperkalemia can cause rhythm disturbances, the predominant feature here is a regular atrial tachycardia with AV block, not T-wave changes typical of electrolyte imbalance. *Ventricular bigeminy* - **Ventricular bigeminy** would manifest as alternating normal QRS complexes with premature ventricular contractions (PVCs). - The ECG shows a narrow complex tachycardia with visible P waves, which are not characteristic of PVCs or ventricular bigeminy. *Non paroxysmal atrial tachycardia with irregular AV block* - Although there is non-paroxysmal atrial tachycardia, the **AV block is regular** (e.g., a consistent 2:1 or 3:1 conduction ratio), not irregular. - An irregular AV block would suggest variability in AV nodal conduction, such as in AV Wenckebach or Mobitz type II with variable conduction, which is not what is seen in this tracing.
Question 3: A 3-year-old child presents with the clinical features shown in the image. What is the most likely diagnosis?
- A. Kawasaki disease (Correct Answer)
- B. Scarlet fever
- C. Kikuchi disease
- D. Rosai-Dorfman disease
Explanation: ***Kawasaki disease*** * The image displays classic signs of **Kawasaki disease**, including **bilateral conjunctivitis without exudates** (top left), **erythema of the palms and soles with desquamation** (top right), **cervical lymphadenopathy** (bottom left, indicated by swelling in the neck region), and a **strawberry tongue** (bottom right). * These clinical features, especially in a young child, are diagnostic for **Kawasaki disease**, which is a vasculitis affecting medium-sized arteries, most notably the coronary arteries. *Scarlet fever* * While **scarlet fever** can cause a **strawberry tongue** and a rash, the rash is typically a **fine, sandpaper-like rash** that blanches with pressure, not usually characterized by the distinct palm/sole erythema and desquamation seen in the image. * **Conjunctivitis** is not a prominent feature of scarlet fever, and the lymphadenopathy is typically less pronounced and may be tender. *Kikuchi disease* * **Kikuchi disease** (histiocytic necrotizing lymphadenitis) primarily presents with **cervical lymphadenopathy, fever**, and often rash, but it does **not typically involve conjunctivitis or changes in the hands, feet, or tongue** as dramatically depicted. * It is a self-limiting condition of unknown etiology, distinct from the systemic vasculitis of Kawasaki disease. *Rosai-Dorfman disease* * **Rosai-Dorfman disease** (sinus histiocytosis with massive lymphadenopathy) is characterized by **massive, painless lymphadenopathy**, particularly cervical, with fever and other systemic symptoms. * However, it does **not present with the specific mucocutaneous findings** of conjunctivitis, strawberry tongue, or characteristic hand/foot changes seen in the images indicative of Kawasaki disease.
Question 4: A 2-year-old epileptic child with developmental delay presents to emergency with fever for the last two days. NCCT shows:
- A. Subdural hemorrhage
- B. Arnold-Chiari malformation
- C. Schizencephaly
- D. Lissencephaly (Correct Answer)
Explanation: ***Lissencephaly*** - The image shows a **smooth brain surface** with **absent or reduced gyri and sulci**, which is characteristic of lissencephaly. - This condition is often associated with **developmental delay** and **epilepsy**, consistent with the child's presentation. *Subdural hemorrhage* - A subdural hemorrhage would appear as a **crescent-shaped collection of blood** between the dura mater and arachnoid mater. - The image does not demonstrate any such blood collection. *Arnold-Chiari malformation* - Arnold-Chiari malformation involves the downward displacement of the **cerebellar tonsils** into the foramen magnum. - While it can cause neurological symptoms, the primary finding in the image is a smooth cerebral cortex, not cerebellar displacement. *Schizencephaly* - Schizencephaly is characterized by **clefts or slits in the cerebral hemispheres** that extend from the pial surface to the ventricles. - The image shows a smooth brain surface rather than distinct full-thickness clefts.
Question 5: Comment on the diagnosis based on the image shown below. (Recent NEET Pattern 2016-17)
- A. Proteus syndrome
- B. Plexiform neurofibromatosis (Correct Answer)
- C. Rhabdomyosarcoma
- D. Malignant fibrous histiocytosis
Explanation: ***Plexiform neurofibromatosis*** - The image exhibits significant facial disfigurement with **nodular and soft tissue overgrowth**, particularly around the eye and midface, consistent with a **plexiform neurofibroma**. - This presentation is a classic feature of **Neurofibromatosis Type 1 (NF1)**, where plexiform neurofibromas can be extensive and cause severe cosmetic and functional issues. *Proteus syndrome* - Proteus syndrome is characterized by **asymmetric overgrowth** of various tissues including bone, skin, and fat, often leading to patchy or mosaic patterns of disproportionate growth. - While it involves overgrowth, the specific appearance in the image with its nodular, bag-like masses is more typical of plexiform neurofibroma than the broader, more generalized overgrowth seen in Proteus syndrome. *Rhabdomyosarcoma* - Rhabdomyosarcoma is a **malignant tumor of skeletal muscle**, typically presenting as a rapidly growing mass. - The lesions in the image appear more chronic and diffuse, lacking the aggressive, distinct tumoral characteristics of a typical rhabdomyosarcoma. *Malignant fibrous histiocytosis* - Malignant fibrous histiocytosis (now often classified under **undifferentiated pleomorphic sarcoma**) is a **high-grade soft tissue sarcoma** primarily affecting older adults, typically presenting as a rapidly enlarging mass. - Similar to rhabdomyosarcoma, this is a distinct malignant tumor and does not match the diffuse, chronic, and somewhat benign-appearing overgrowth seen in the picture.
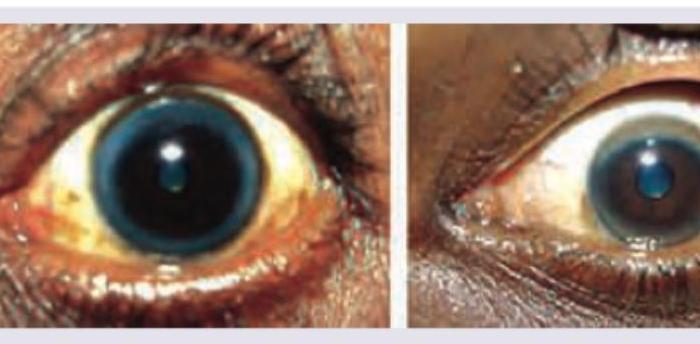
Question 6: Which of the following is correct about the image shown? (Recent NEET Pattern 2016-17)
- A. A = Arcus senilis, B = Kayser-Fleischer ring
- B. A = Kayser Fleischer ring, B = Arcus senilis (Correct Answer)
- C. A = Arcus senilis, B = Hudson-Stahli line
- D. A = Hudson-Stahli line, B = Arcus senilis
Explanation: ***A = Kayser Fleischer ring, B = Arcus senilis*** - Image A displays a **Kayser-Fleischer ring**, a greenish-brown ring in the periphery of the cornea, characteristic of **Wilson's disease** due to copper deposition. - Image B shows **arcus senilis**, a milky-white or grayish ring around the cornea, which is a **common age-related change** due to lipid deposits, and can appear at any age. *A = Arcus senilis, B = Kayser-Fleischer ring* - This option incorrectly identifies the lesions; the ring in image A is associated with copper deposition, not lipid deposition. - The ring in image B is clearly a common lipid ring often seen in older individuals, contrasting with the distinct appearance of a Kayser-Fleischer ring. *A = Arcus senilis, B = Hudson-Stahli line* - Image A does not show arcus senilis; its color and location are consistent with copper deposition. - Image B does not depict a Hudson-Stahli line, which is a thin, brownish-linear deposit of iron in the corneal epithelium, typically horizontal and not circumferential. *A = Hudson-Stahli line, B = Arcus senilis* - Image A's appearance, as a circumferential greenish-brown deposit, is not consistent with a linear Hudson-Stahli line. - While image B correctly identifies arcus senilis, the identification of A as a Hudson-Stahli line is incorrect.
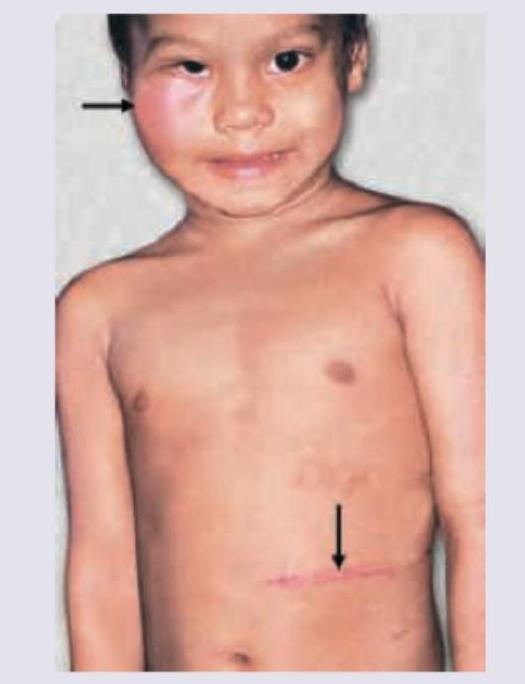
Question 7: Comment on the diagnosis of this child, presenting with eye swelling. (Recent NEET Pattern 2016-17)
- A. Chloroma
- B. Neuroblastoma (Correct Answer)
- C. Wilms tumor
- D. Ameloblastoma
Explanation: ***Neuroblastoma*** - The image shows **periorbital ecchymosis** and **proptosis** in a child, which are classic signs of orbital metastatic neuroblastoma, often referred to as "raccoon eyes." - The abdominal scar suggests a prior surgery, possibly for removal of the primary tumor, which is typically found in the **adrenal gland** or **sympathetic ganglia**. *Chloroma* - **Chloromas** (also known as granulocytic sarcomas) are extramedullary manifestations of myeloid leukemia, presenting as solid tumors composed of myeloid blast cells. - While they can appear in the orbit and mimic proptosis, the presence of bilateral periorbital ecchymosis ("raccoon eyes") is more characteristic of neuroblastoma metastasis. *Wilms tumor* - **Wilms tumor** is a kidney cancer, typically presenting as an **abdominal mass** and occasionally with hypertension or hematuria. - Ocular manifestations, such as proptosis, are extremely **rare** and do not typically involve periorbital ecchymosis. *Ameloblastoma* - An **ameloblastoma** is a benign but locally aggressive tumor of odontogenic (tooth-forming) origin, primarily affecting the **jawbones**. - It does not metastasize to the orbit and would not present with periorbital swelling or ecchymosis.
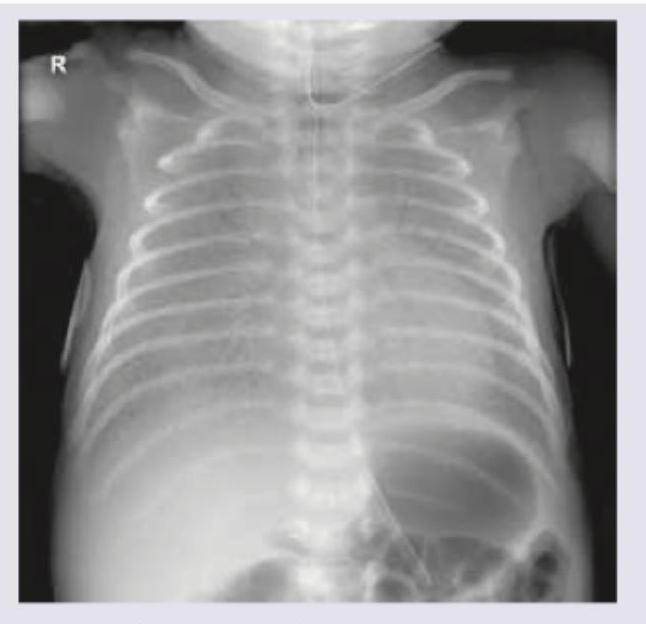
Question 8: Neonate born at 34 weeks with premature rupture of membranes develops respiratory distress. CXR was performed. All are considered in differential diagnosis except:
- A. Congenital pneumonia
- B. Hyaline membrane disease
- C. Congenital alveolar proteinosis
- D. Tetralogy of Fallot (Correct Answer)
Explanation: ***Tetralogy of Fallot*** - **Tetralogy of Fallot** is a **cyanotic congenital heart defect** characterized by VSD, pulmonary stenosis, right ventricular hypertrophy, and overriding aorta. - It presents primarily with **cyanosis** (not respiratory distress) and would show **normal or oligemic lung fields** on CXR, not the diffuse parenchymal lung disease patterns seen in RDS, pneumonia, or alveolar proteinosis. - **Not part of the differential diagnosis** for a preterm neonate with PROM presenting with respiratory distress and lung infiltrates on imaging. *Congenital pneumonia* - This is a significant concern in a neonate born prematurely with **premature rupture of membranes (PROM)**, as ascending infection is a known risk factor. - Chest X-ray findings can include **diffuse hazy infiltrates** or **patchy consolidation**, consistent with infections. - Would be considered in the differential diagnosis. *Hyaline membrane disease* - Also known as **respiratory distress syndrome (RDS)**, this is common in **premature infants at 34 weeks** due to **surfactant deficiency**. - The chest X-ray typically shows **diffuse reticulogranular ground-glass opacities** and **air bronchograms**. - Most common cause of respiratory distress in preterm neonates and a key differential. *Congenital alveolar proteinosis* - This is a rare genetic disorder where **surfactant proteins accumulate in the alveoli**, leading to impaired gas exchange and respiratory distress. - Chest X-ray findings often include **diffuse alveolar infiltrates** or consolidation, which can resemble other neonatal lung diseases. - Though rare, must be considered in the differential for neonatal respiratory distress.
Question 9: Preterm child on cow milk due to death of mother is having blood in stools. X-ray abdomen was done. Diagnosis is:
- A. Rigler sign (Correct Answer)
- B. Double bubble appearance
- C. Claw sign
- D. Bird of prey sign
Explanation: ***Rigler sign*** - Rigler sign (also called **double wall sign**) refers to **visualization of both sides of the bowel wall** on X-ray due to **free intraperitoneal air (pneumoperitoneum)**, indicating bowel perforation. - In the clinical context of a **preterm infant on cow milk with bloody stools**, this presentation is highly suggestive of **Necrotizing Enterocolitis (NEC) with perforation**. - The X-ray shows Rigler sign as evidence of pneumoperitoneum, a serious complication of NEC requiring urgent surgical intervention. - **Key NEC radiological findings** include: pneumatosis intestinalis (intramural gas), portal venous gas, and pneumoperitoneum (Rigler sign) in cases with perforation. *Double bubble appearance* - This sign shows **two distinct air-filled structures** (distended stomach and duodenum) on abdominal X-ray, indicating **duodenal obstruction** from duodenal atresia or annular pancreas. - Not associated with bloody stools or NEC in preterm infants. *Claw sign* - The claw sign is seen in **intussusception**, where the bowel telescopes into itself, creating a soft tissue mass with a crescent-shaped gas pattern. - Typically occurs in older infants (6-18 months), not preterm neonates, and presents differently from NEC. *Bird of prey sign* - This sign is associated with **sigmoid or cecal volvulus**, showing a distended bowel loop with a beak-like configuration. - Represents large bowel obstruction, not the typical presentation of a preterm infant with feeding intolerance and bloody stools from NEC.
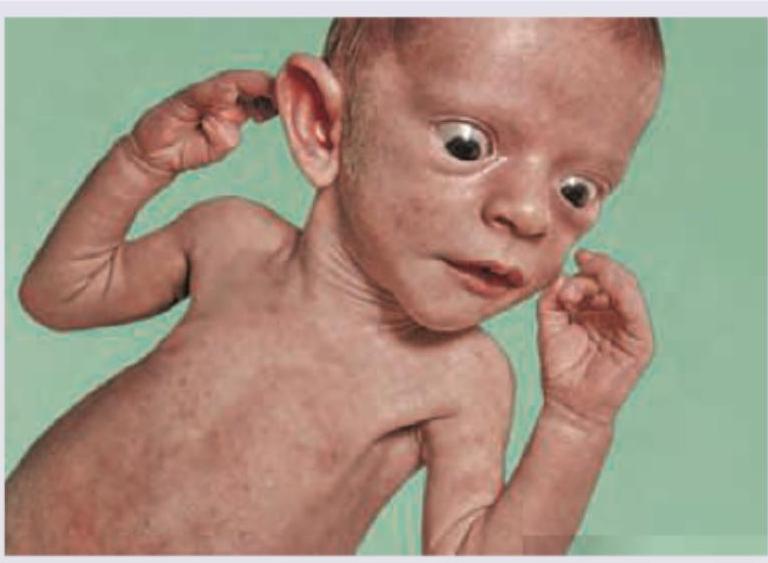
Question 10: Which of the following is the best diagnosis of this neonate who is excessively hungry, warm with flushed skin?
- A. Neonatal thyrotoxicosis (Correct Answer)
- B. Neonatal lupus
- C. Congenital hypothyroidism
- D. Progeria
Explanation: ***Neonatal thyrotoxicosis*** - The image shows a neonate with **exophthalmos** and signs of being **hypermetabolic** (excessively hungry, warm, flushed skin), all consistent with hyperthyroidism. - This condition occurs when **maternal thyroid-stimulating immunoglobulins** cross the placenta, causing transient hyperthyroidism in the newborn. *Neonatal lupus* - Neonatal lupus is primarily characterized by **congenital heart block** and **dermatological manifestations** (e.g., erythematous annular lesions) but does not typically present with severe metabolic hyperactivity or exophthalmos as seen here. - It is caused by the transplacental passage of maternal autoantibodies (anti-Ro/SSA and anti-La/SSB). *Congenital hypothyroidism* - Congenital hypothyroidism would present with symptoms opposite to those described, such as **lethargy**, **poor feeding**, **cold and mottled skin**, and **constipation**. - Physical features often include a **puffy face**, **macroglossia**, and an **umbilical hernia**. *Progeria* - Progeria is a rare genetic disorder characterized by **accelerated aging** that typically manifests later in infancy or early childhood with features like **alopecia**, **thin skin**, and **skeletal abnormalities**, which are not depicted or described as primary symptoms here. - It does not cause the acute signs of hypermetabolism seen in neonatal thyrotoxicosis.