NEET-PG 2017 — Pathology
14 Previous Year Questions with Answers & Explanations
A 70-year-old man presents with painless cervical lymphadenopathy with progressive pallor and petechiae on ankles. Peripheral smear shows presence of:
The following bone marrow specimen is suggestive of diagnosis of:
Identify the cell.
Name the test given.

Name the anticoagulant used in the following method.
The resected specimen of a kidney is seen below. What is the diagnosis?

Comment on type of glomerulonephritis present in the kidney biopsy slide. (Recent NEET Pattern 2016-17)
All are causes of this glomerular presentation except: (Recent NEET Pattern 2016-17)
All are true about the presentation in kidney biopsy shown except: (Recent NEET Pattern 2016-17)
Comment on the diagnosis of light microscopy finding in kidney biopsy. (Recent NEET Pattern 2016-17)
NEET-PG 2017 - Pathology NEET-PG Practice Questions and MCQs
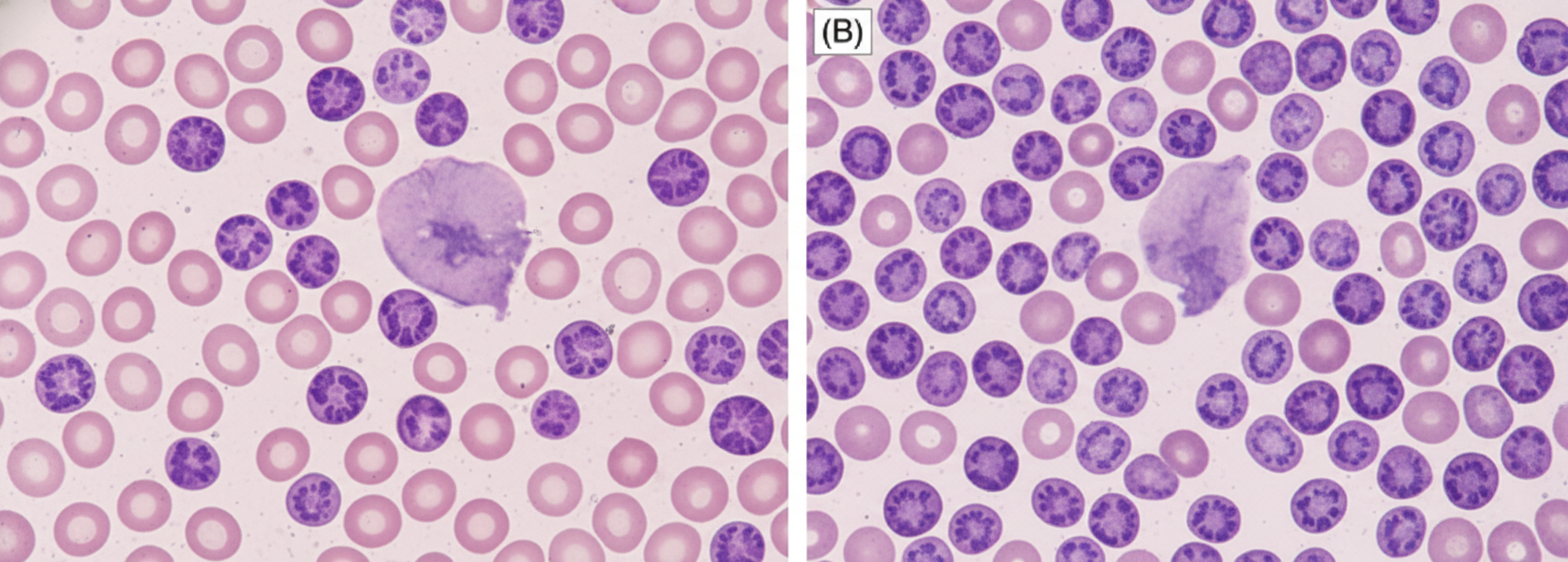
Question 1: A 70-year-old man presents with painless cervical lymphadenopathy with progressive pallor and petechiae on ankles. Peripheral smear shows presence of:
- A. Acute ITP
- B. Chronic ITP
- C. CLL (Correct Answer)
- D. Richter syndrome
- E. Hairy cell leukemia
Explanation: ***CLL*** - The presentation of **painless cervical lymphadenopathy**, progressive **pallor** (due to anemia), and **petechiae** (due to thrombocytopenia) in an elderly patient is highly suggestive of **Chronic Lymphocytic Leukemia (CLL)** [2]. - Peripheral smear in CLL typically shows a proliferation of mature-appearing **small lymphocytes** and characteristic **smudge cells** [1]. *Acute ITP* - Acute ITP is characterized by sudden onset of **thrombocytopenia** and bleeding, often following a viral infection, and is more common in children. - It does not typically present with **lymphadenopathy** or progressive pallor as a primary feature. *Chronic ITP* - Chronic ITP is characterized by isolated **thrombocytopenia** and bleeding symptoms, usually without lymphadenopathy or significant anemia unless bleeding is severe. - The presence of **lymphadenopathy** points away from isolated ITP and towards a systemic hematological malignancy. *Richter syndrome* - Richter syndrome is the transformation of CLL into a more aggressive lymphoma, most commonly **diffuse large B-cell lymphoma (DLBCL)**. - While it can present with rapidly enlarging lymph nodes and systemic symptoms, the initial presentation described (painless lymphadenopathy, progressive pallor, petechiae) is more typical of **untreated CLL** before transformation [2]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, p. 602. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 612-613.
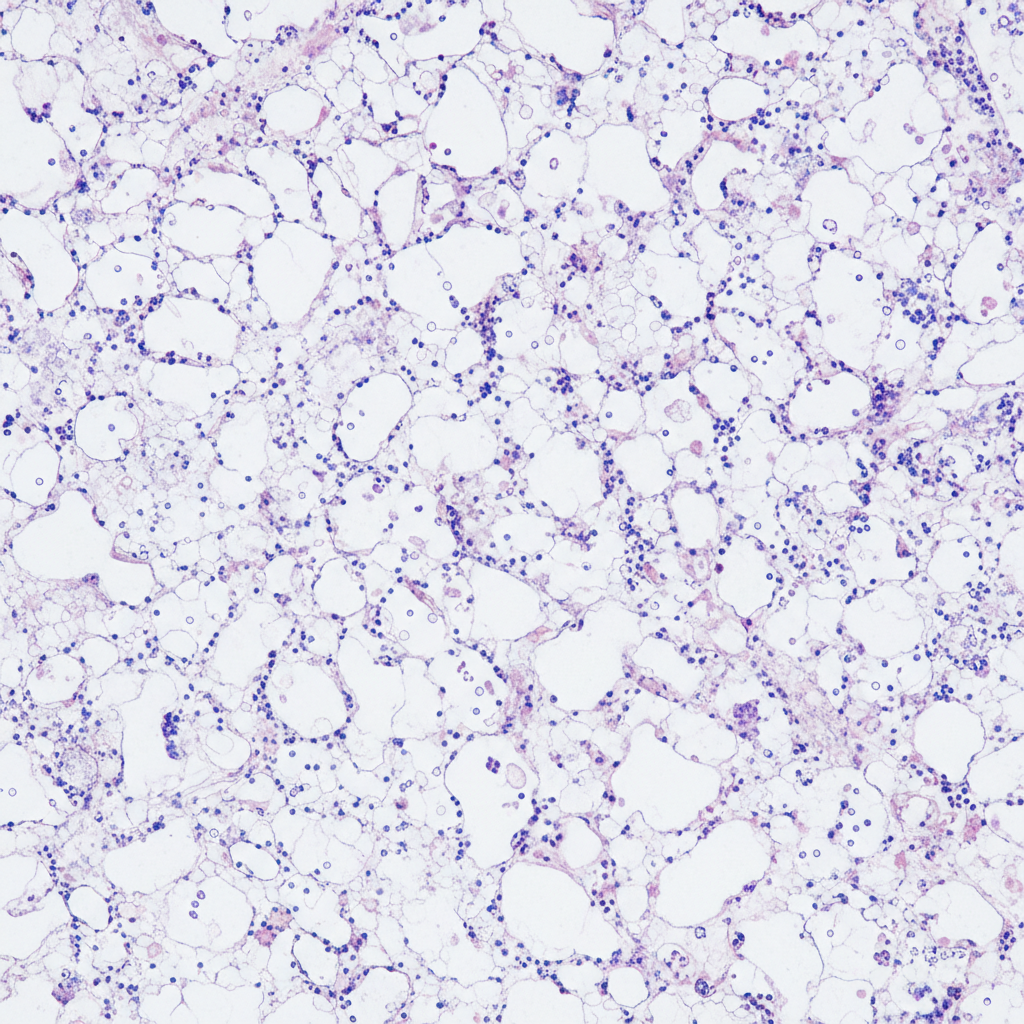
Question 2: The following bone marrow specimen is suggestive of diagnosis of:
- A. Pure red cell aplasia
- B. Myelodysplasia
- C. Normal marrow
- D. Aplastic anemia (Correct Answer)
- E. Hairy cell leukemia
Explanation: ***Aplastic anemia*** - Aplastic anemia is characterized by a **hypocellular bone marrow** with a significant reduction in hematopoietic cells and replacement by **fat cells (adipocytes)** as seen in the specimen. - This condition leads to **pancytopenia**, affecting all three cell lines (red blood cells, white blood cells, and platelets). - Bone marrow cellularity is typically **<25%** (normal ~50%), with the remaining space occupied by fat and stroma. *Pure red cell aplasia* - Pure red cell aplasia primarily affects **erythroid precursors** in the bone marrow, leading to severe anemia. - Unlike aplastic anemia, the **myeloid and megakaryocytic lineages** are typically preserved, and overall marrow cellularity is not severely reduced. *Myelodysplasia* - Myelodysplastic syndromes (MDS) are characterized by **dysplastic changes** in one or more hematopoietic cell lines and **ineffective hematopoiesis**. - The bone marrow in MDS can be **normocellular or hypercellular** with morphological dysplasia (abnormal cell forms), not simply hypocellular with fat replacement. *Normal marrow* - A normal bone marrow is **cellular for the patient's age**, with a healthy mix of hematopoietic cells from all lineages and appropriate fat content (~50% cellularity in adults). - It would not show the profound **hypocellularity and fat replacement** seen in the provided specimen. *Hairy cell leukemia* - Hairy cell leukemia (HCL) shows bone marrow infiltration by **lymphoid cells with characteristic cytoplasmic hair-like projections** (best seen on peripheral smear). - Bone marrow biopsy in HCL typically shows **"fried egg" appearance** due to widely spaced hairy cells with pale cytoplasm — not a simple hypocellular, fat-replaced marrow. - HCL causes **dry tap** on aspiration but the trephine shows infiltration, not the pure hypocellularity seen in aplastic anemia. **References:** [1] Kumar V, Abbas AK, et al. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Red Blood Cell and Bleeding Disorders, p. 662. [2] Kumar V, Abbas AK, et al. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Red Blood Cell and Bleeding Disorders, pp. 662-663. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 595-596. [4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 613-614.
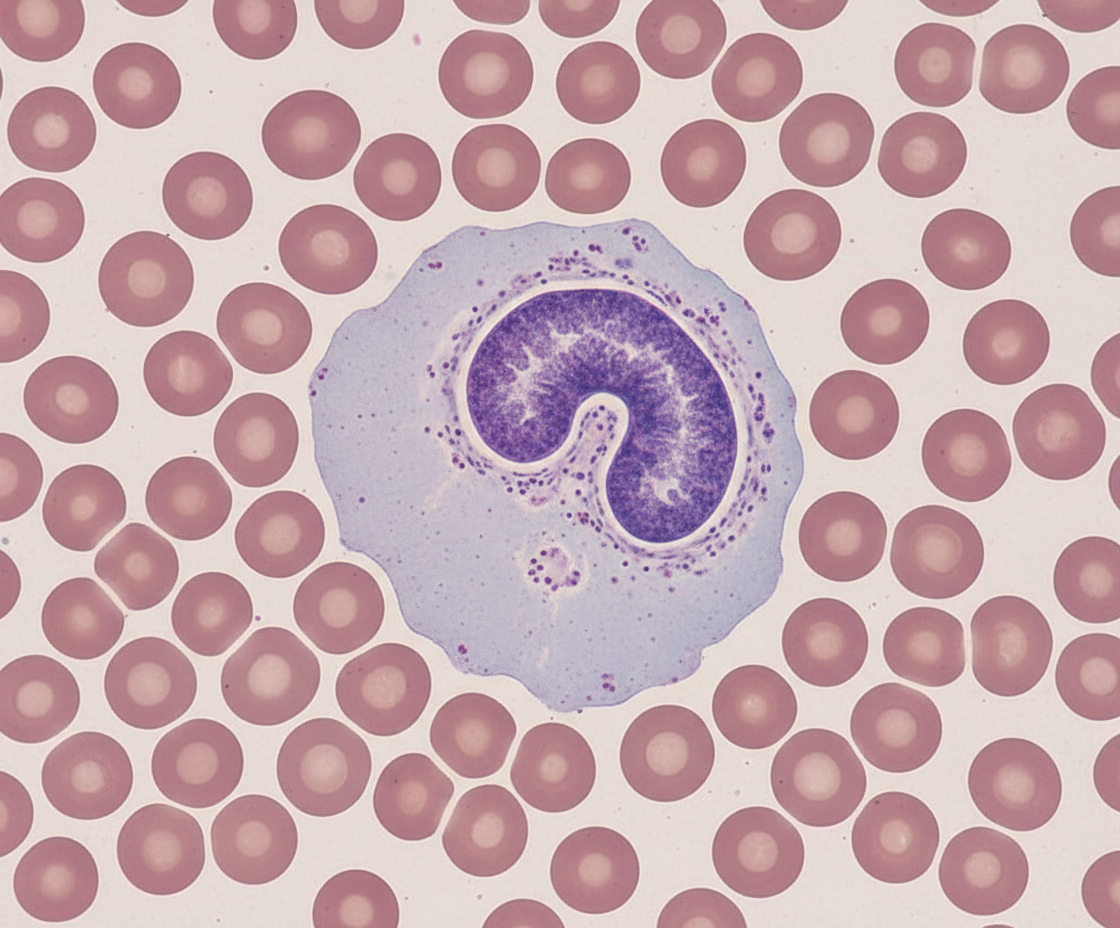
Question 3: Identify the cell.
- A. Eosinophil
- B. Basophil
- C. Monocyte (Correct Answer)
- D. Lymphocyte
- E. Neutrophil
Explanation: ***Monocyte*** - Monocytes are characterized by their **large size** (12-20 µm), **kidney-shaped or horseshoe-shaped nucleus**, and **abundant, often grayish-blue cytoplasm** with fine azurophilic granules [1]. - They are precursors to **macrophages** and play a crucial role in phagocytosis and antigen presentation [1]. *Eosinophil* - Eosinophils have a **bilobed nucleus** and prominent **red-orange granules** in their cytoplasm, which stain with eosin [1]. - They are primarily involved in allergic reactions and defense against **parasitic infections** [1]. *Basophil* - Basophils are characterized by a **lobed nucleus** often obscured by large, coarse, **dark purple-blue granules** that contain histamine and heparin [1]. - They are the least common granulocyte and are involved in **allergic and inflammatory responses** [1]. *Lymphocyte* - Lymphocytes are typically **smaller** than monocytes, with a **large, round, or slightly indented nucleus** that occupies most of the cell [1]. - Their cytoplasm is usually **scanty and pale blue**, often appearing as a thin rim around the nucleus [1]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 578-580.
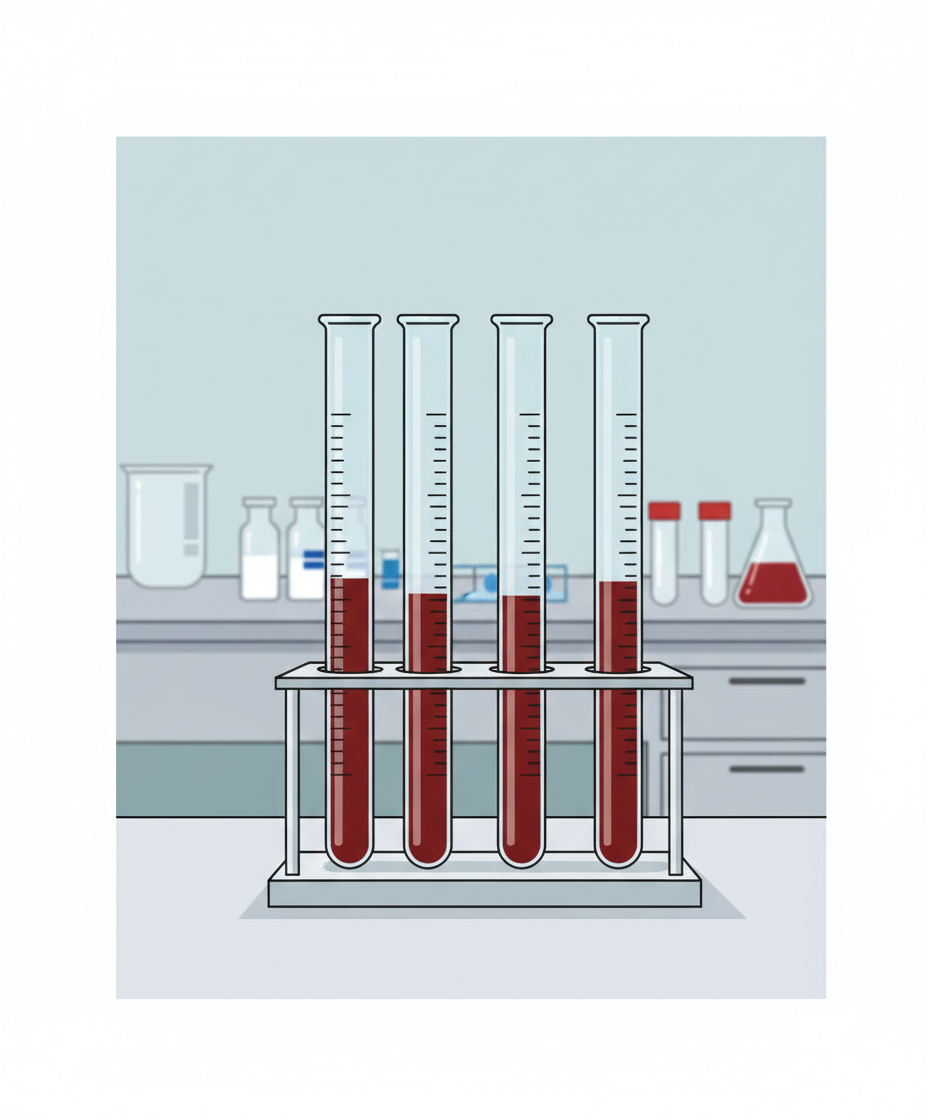
Question 4: Name the test given.
- A. Osmotic fragility
- B. NESTROFT
- C. Sickling test
- D. ESR measurement (Correct Answer)
- E. Packed cell volume (PCV)
Explanation: ***ESR measurement*** - The image displays a **Westergren tube** with a column of blood, showing distinct layers of plasma on top and red blood cells settled below against a calibrated scale. - This setup is characteristic of an **Erythrocyte Sedimentation Rate (ESR)** test, which measures the rate at which red blood cells fall in a standardized tube over a specific time, indicating inflammation. *Osmotic fragility* - This test involves exposing red blood cells to varying concentrations of **hypotonic saline solutions** to assess their resistance to lysis. - The results are typically reported as a curve showing the percentage of hemolysis at different saline concentrations, not a simple sedimentation in a tube. *NESTROFT* - The **Naked Eye Single Tube Red Cell Osmotic Fragility Test (NESTROFT)** is a quick screening test for **beta-thalassemia trait**. - It involves mixing blood with a hypotonic saline solution and observing for complete hemolysis or partial hemolysis with a button of red cells, which is different from the image shown. *Sickling test* - A sickling test is used to detect the presence of **sickle hemoglobin**, which causes red blood cells to deform into a sickle shape under low oxygen conditions. - This test is usually performed by adding a reducing agent like **sodium metabisulfite** to a blood sample and observing cell morphology under a microscope or by turbidity, not by sedimentation in a calibrated tube. *Packed cell volume (PCV)* - PCV or **hematocrit** measures the proportion of blood volume occupied by red blood cells after centrifugation in a **microhematocrit tube**. - While it does involve blood in a tube, the tube is much smaller (capillary tube) and requires **centrifugation** to separate components, unlike ESR which relies on natural sedimentation under gravity in a larger calibrated Westergren tube.
Question 5: Name the anticoagulant used in the following method.
- A. EDTA
- B. Heparin
- C. Trisodium citrate (Correct Answer)
- D. Dalteparin
- E. Sodium fluoride
Explanation: ***Trisodium citrate*** - The image displays a method for measuring **Erythrocyte Sedimentation Rate (ESR)**, typically performed using the **Westergren method**. - In the Westergren method, **trisodium citrate** is the standard anticoagulant used to prevent blood coagulation, allowing red blood cells to settle over time. *EDTA* - **EDTA (ethylenediaminetetraacetic acid)** is a common anticoagulant, primarily used for **hematology tests** such as complete blood counts (CBC), as it preserves cell morphology. - While it prevents clotting, it is not the standard anticoagulant for the Westergren ESR method, as it can cause red blood cell shrinkage affecting sedimentation. *Heparin* - **Heparin** acts as an anticoagulant by enhancing the activity of **antithrombin III**, and is commonly used for chemistry and general coagulation studies. - It interferes with the sedimentation rate in ESR measurements, making it unsuitable for this specific test. *Dalteparin* - **Dalteparin** is a type of **low molecular weight heparin (LMWH)** used therapeutically as an anticoagulant to prevent and treat blood clots. - It is not used as an in-vitro anticoagulant for blood collection tubes or lab diagnostic tests like ESR. *Sodium fluoride* - **Sodium fluoride** is an anticoagulant and enzymatic inhibitor primarily used for **glucose measurement**, as it inhibits glycolysis and preserves glucose levels. - It is not appropriate for ESR testing, as it does not provide the optimal conditions for red blood cell sedimentation measurement.
Question 6: The resected specimen of a kidney is seen below. What is the diagnosis?
- A. Amyloidosis
- B. Acute poststreptococcal glomerulonephritis
- C. Flea bitten kidney of malignant hypertension (Correct Answer)
- D. Chronic glomerulonephritis
- E. Acute tubular necrosis
Explanation: ***Flea bitten kidney of malignant hypertension*** - The term "flea-bitten kidney" describes the gross appearance of the kidney in **malignant hypertension**, characterized by numerous pinpoint hemorrhages on the cortical surface [1]. - These hemorrhages result from the rupture of **arterioles and capillaries** due to severe, uncontrolled high blood pressure [1]. *Amyloidosis* - In **amyloidosis**, the kidneys typically appear enlarged, pale, and waxy due to the deposition of **amyloid protein**. - It does not typically present with the characteristic pinpoint hemorrhages seen in a "flea-bitten" appearance. *Acute poststreptococcal glomerulonephritis* - In **acute poststreptococcal glomerulonephritis (APSGN)**, the kidneys are usually enlarged and pale, often with a smooth surface. - While there can be some congestion, the classic "flea-bitten" appearance with widespread petechial hemorrhages is not a typical gross finding. *Chronic glomerulonephritis* - **Chronic glomerulonephritis** typically leads to shrunken, granular, and scarred kidneys due to long-standing inflammation and fibrosis. - The gross appearance is usually one of atrophy and scarring, not the acute hemorrhagic spots described as "flea-bitten." **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, p. 945.
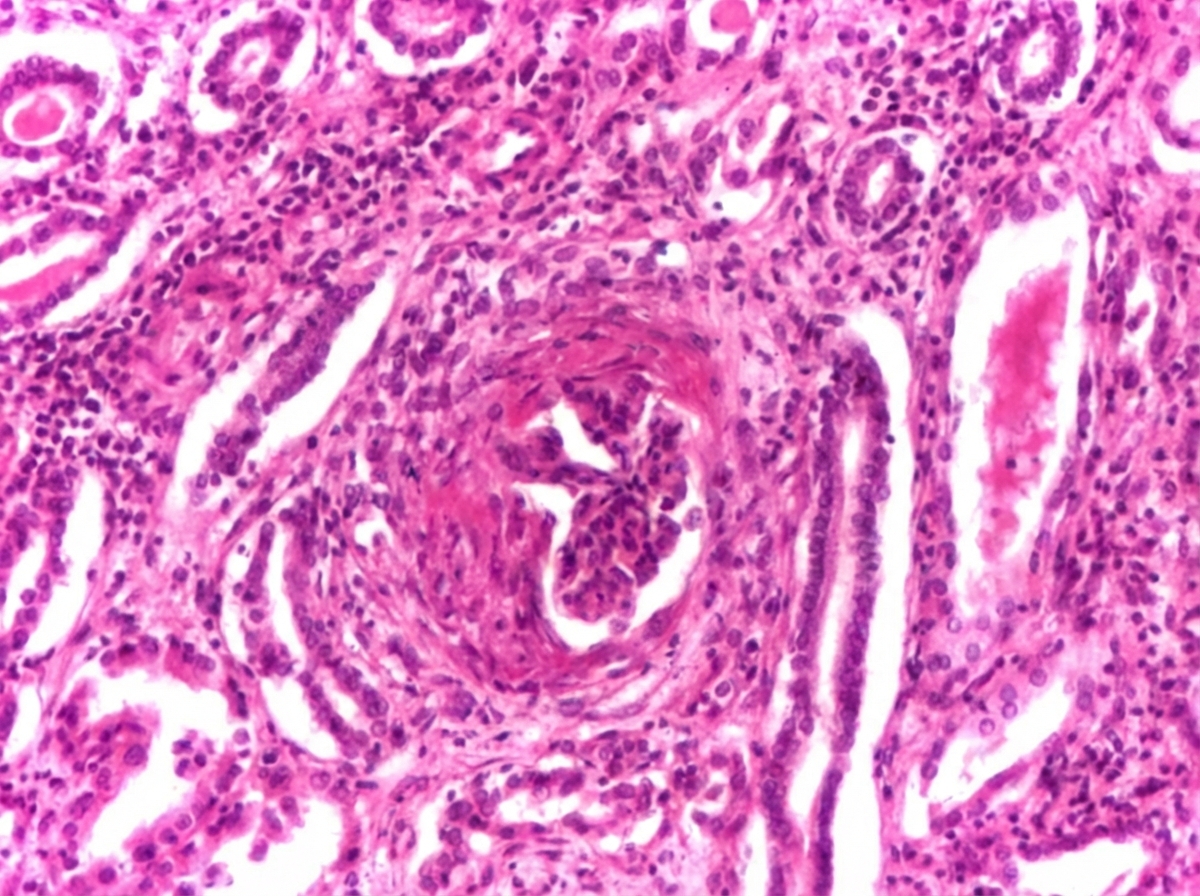
Question 7: Comment on type of glomerulonephritis present in the kidney biopsy slide. (Recent NEET Pattern 2016-17)
- A. Acute glomerulonephritis
- B. Crescentic glomerulonephritis (Correct Answer)
- C. Focal segmental glomerulosclerosis
- D. Diffuse glomerulosclerosis
- E. Membranous glomerulonephritis
Explanation: ***Crescentic glomerulonephritis*** - The presence of **crescents** in the glomeruli is the hallmark of **crescentic glomerulonephritis**, indicating severe glomerular injury [1]. - Crescents are formed by the proliferation of **parietal epithelial cells** and infiltration of macrophages, leading to rapid decline in renal function [1]. *Acute glomerulonephritis* - This is a broad term that can encompass various forms of glomerulonephritis, but it does not specifically describe the **morphological finding of crescents**. - Acute glomerulonephritis often presents with **nephritic syndrome** (hematuria, proteinuria, hypertension), but the biopsy finding of crescents is more specific [1]. *Focal segmental glomerulosclerosis* - Characterized by **sclerosis** (scarring) affecting **some glomeruli** (focal) and **only parts of the glomerular tuft** (segmental). - It typically presents with **nephrotic syndrome** (heavy proteinuria, edema, hypoalbuminemia), which is distinct from the rapid renal failure seen with crescents. *Diffuse glomerulosclerosis* - This term implies widespread **sclerosis** affecting **all glomeruli**, often seen in advanced chronic kidney disease. - It does not specifically describe the **active inflammatory process** and crescent formation characteristic of crescentic glomerulonephritis [2]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 528-529. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 536-537.
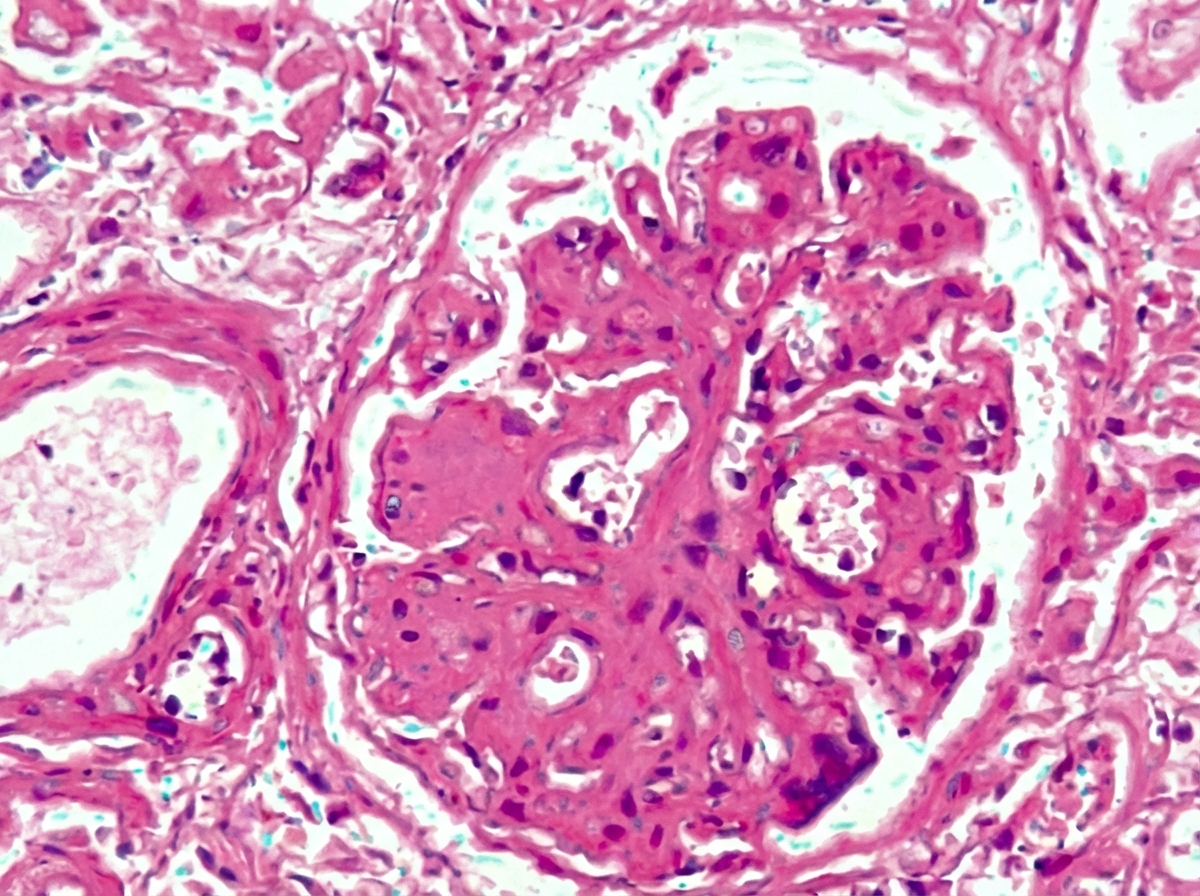
Question 8: All are causes of this glomerular presentation except: (Recent NEET Pattern 2016-17)
- A. HIV
- B. Reflux nephropathy (Correct Answer)
- C. Hepatitis B
- D. Heroin abuse
- E. Obesity
Explanation: ***Reflux nephropathy*** - This condition primarily causes **tubulointerstitial damage** and **scarring**, leading to chronic kidney disease, but it is not a direct cause of a primary glomerular presentation like **focal segmental glomerulosclerosis (FSGS)**. - While it can lead to proteinuria, it's usually due to secondary glomerular changes from chronic damage rather than a primary glomerular disease. *HIV* - **HIV-associated nephropathy (HIVAN)** is a common cause of **collapsing FSGS**, a specific glomerular presentation [1] [2]. - It is characterized by rapid progression to end-stage renal disease and often presents with heavy proteinuria [1]. *Hepatitis B* - Hepatitis B infection is strongly associated with **membranous nephropathy** and, less commonly, with **membranoproliferative glomerulonephritis (MPGN)**, both of which are distinct glomerular presentations [1]. - These conditions involve immune complex deposition in the glomeruli. *Heroin abuse* - Heroin abuse is a well-known cause of **focal segmental glomerulosclerosis (FSGS)**, often presenting as **heroin-associated nephropathy** [3] [4]. - This condition typically leads to significant proteinuria and progressive renal failure [3] [4]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 531-532. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 924-925. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 927-928. [4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 530-531.
Question 9: All are true about the presentation in kidney biopsy shown except: (Recent NEET Pattern 2016-17)
- A. Loss of foot processes
- B. IgG and properdin deposits (Correct Answer)
- C. Hyalinosis
- D. Seen with HIV associated nephropathy
- E. Presents with nephrotic syndrome
Explanation: ***IgG and properdin deposits*** - The question asks for what is *not* true about the presentation in a kidney biopsy. **IgG and properdin deposits** are characteristic of **dense deposit disease (DDD)** or C3 glomerulopathy, not typically seen in the context of **focal segmental glomerulosclerosis (FSGS)**, which is often implied by the other options. - FSGS is primarily a podocyte disorder, and while immune deposits can occur, IgG and properdin are not its defining immunofluorescence features. In FSGS, immunofluorescence is negative other than non-specific trapping of IgM and C3 in the segmental lesions [1]. The diagnosis requires absence of immune deposits on IF [4]. *Loss of foot processes* - **Loss of foot processes** (podocyte effacement) is a hallmark ultrastructural finding in conditions causing **proteinuria**, including **focal segmental glomerulosclerosis (FSGS)** and minimal change disease [1][3]. - This morphological change is directly responsible for increased glomerular permeability to proteins. Podocyte injury is an underlying mechanism of proteinuria in FSGS [3]. *Hyalinosis* - **Hyalinosis** refers to the accumulation of homogeneous, eosinophilic material, often plasma proteins, within the glomerulus. - It is a characteristic feature of **focal segmental glomerulosclerosis (FSGS)**, particularly in the sclerotic segments, with segmental obliteration of glomerular capillary tufts by sclerosis frequently accompanied by hyalinosis [1]. *Seen with HIV associated nephropathy* - **HIV-associated nephropathy (HIVAN)** is a specific form of **collapsing focal segmental glomerulosclerosis (FSGS)** [1][2]. - It is characterized by prominent tubular microcysts and severe interstitial inflammation and fibrosis, in addition to the collapsing glomerular lesions. FSGS may be secondary to infection such as HIV [3], and the collapsing variant has an unfavorable course [2]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 531-532. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 924-925. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 927-928. [4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 530-531.
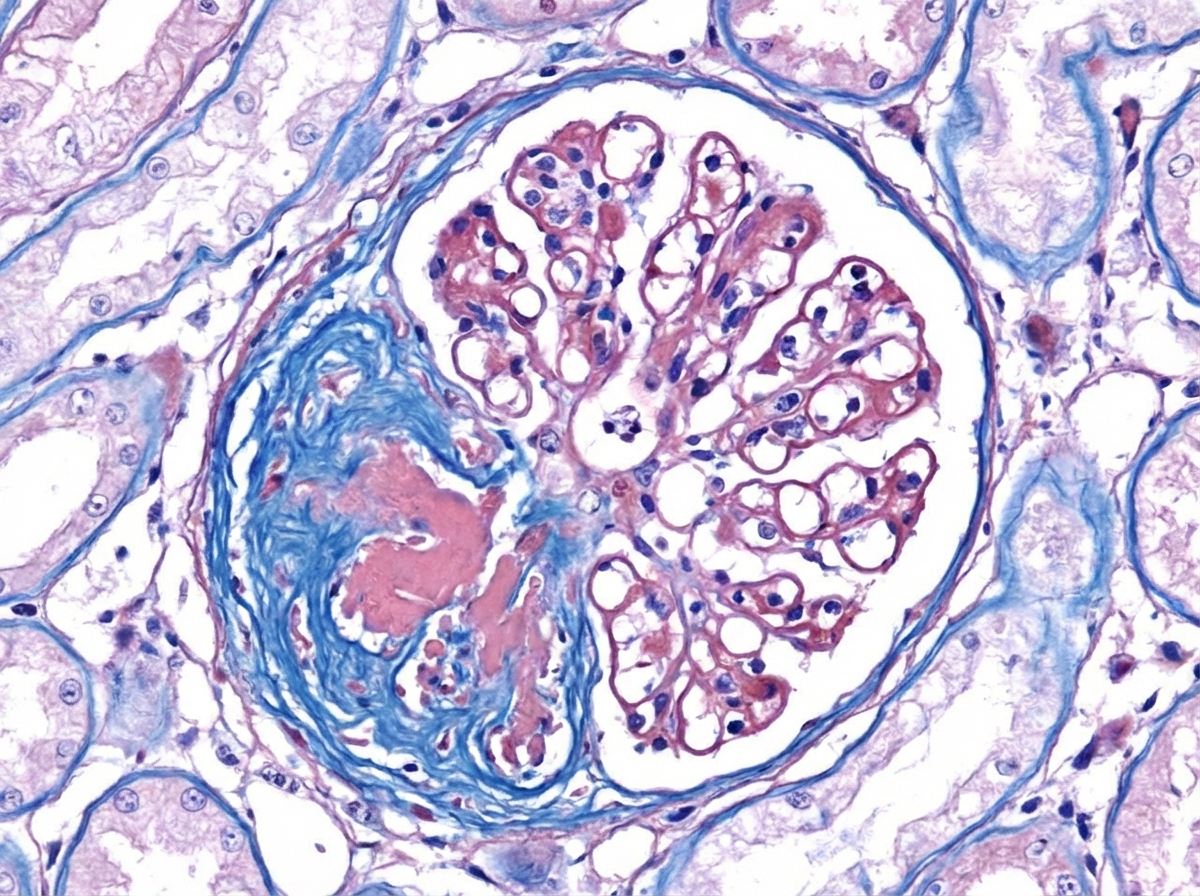
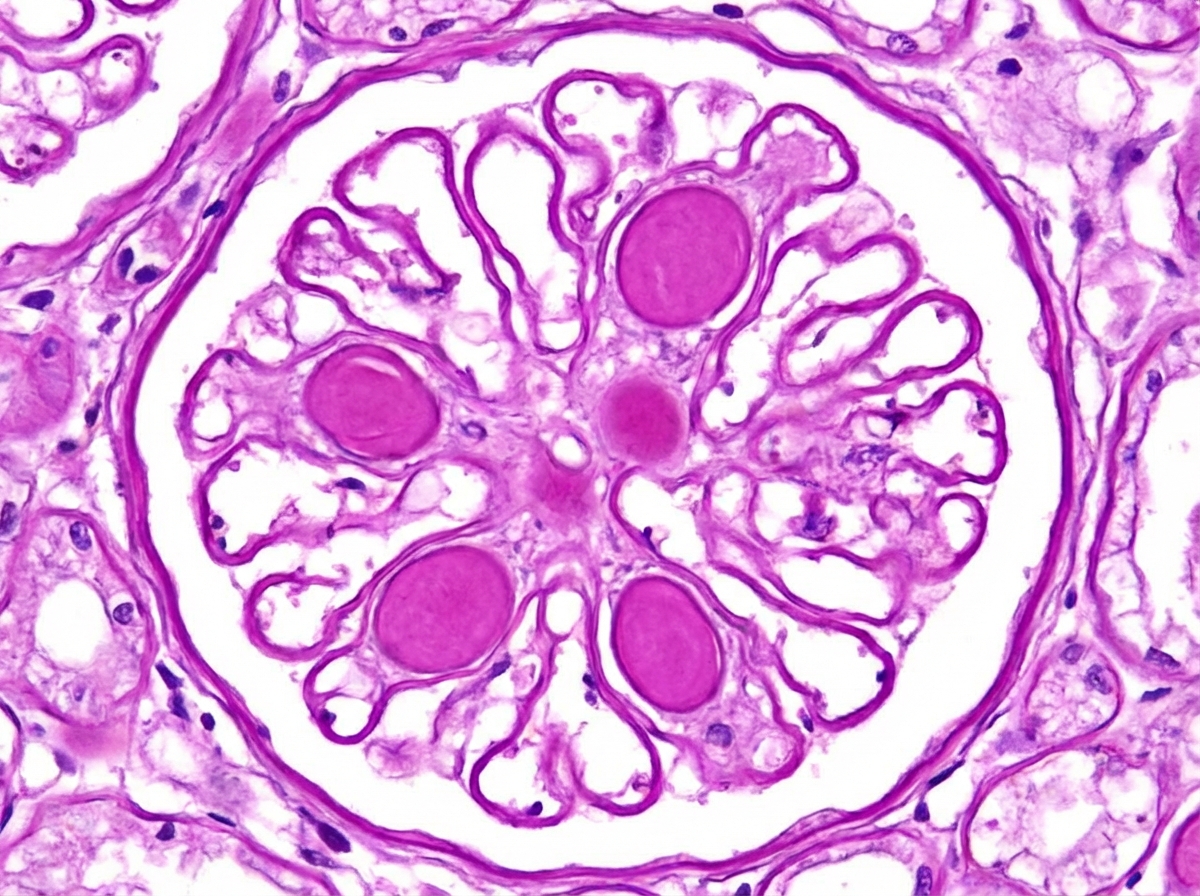
Question 10: Comment on the diagnosis of light microscopy finding in kidney biopsy. (Recent NEET Pattern 2016-17)
- A. Focal segmental glomerulosclerosis
- B. Diffuse glomerulosclerosis
- C. Nodular glomerulosclerosis (Correct Answer)
- D. Minimal change disease
- E. Membranoproliferative glomerulonephritis
Explanation: ***Nodular glomerulosclerosis*** - This finding is characteristic of **diabetic nephropathy**, specifically the **Kimmelstiel-Wilson lesions** [1]. - It involves the formation of **nodular deposits** in the mesangium, leading to glomerulosclerosis. *Focal segmental glomerulosclerosis* - Characterized by **sclerosis** affecting only **some glomeruli** (focal) and only **parts of the glomerular tuft** (segmental). - It is a common cause of **nephrotic syndrome** and is often associated with HIV, heroin abuse, or genetic mutations. *Diffuse glomerulosclerosis* - Implies widespread sclerosis affecting **most or all glomeruli diffusely**. - This is a general term and can be seen in various end-stage renal diseases, not specific to a single primary diagnosis like nodular glomerulosclerosis. *Minimal change disease* - On light microscopy, the glomeruli appear **normal**, hence the term "minimal change" [2]. - The characteristic finding is **effacement of foot processes** on electron microscopy [2], and it is a common cause of nephrotic syndrome in children. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, p. 1121. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Kidney, pp. 922-923.