All (368)Anatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q81
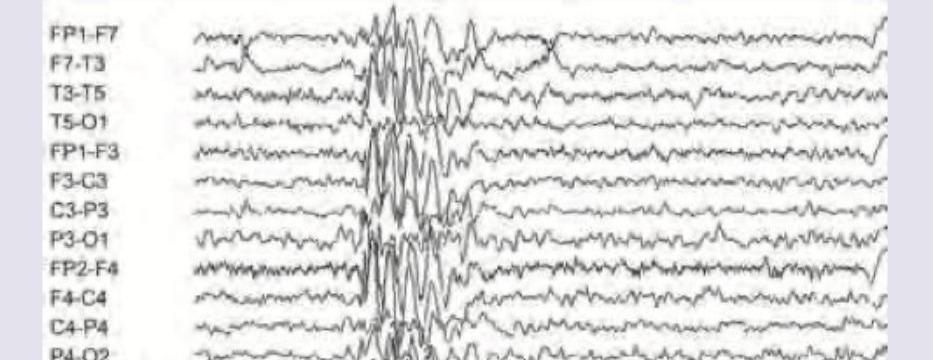
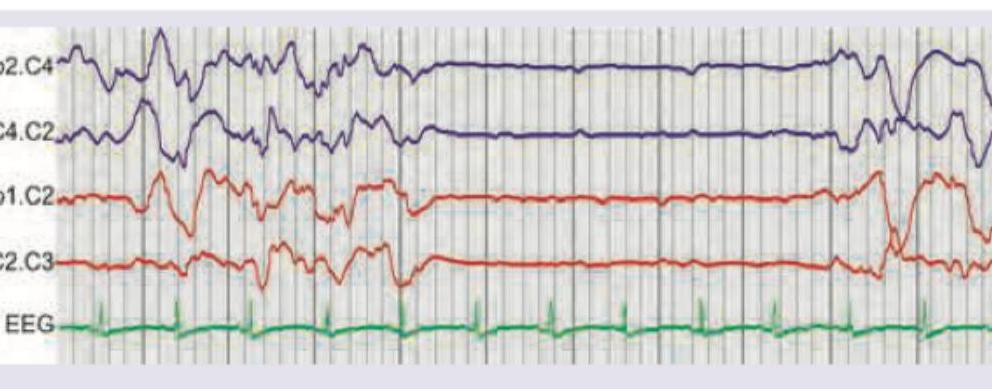
The EEG of the patient shows which of the following? (Recent NEET Pattern 2016-17)
Q82
The EEG of a 16-year-old boy with early morning involuntary movements of hands in his sleep noticed by parents, was performed. Immunization is complete. What does EEG show? (Recent NEET Pattern 2016-17)