All (368)Anatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q51
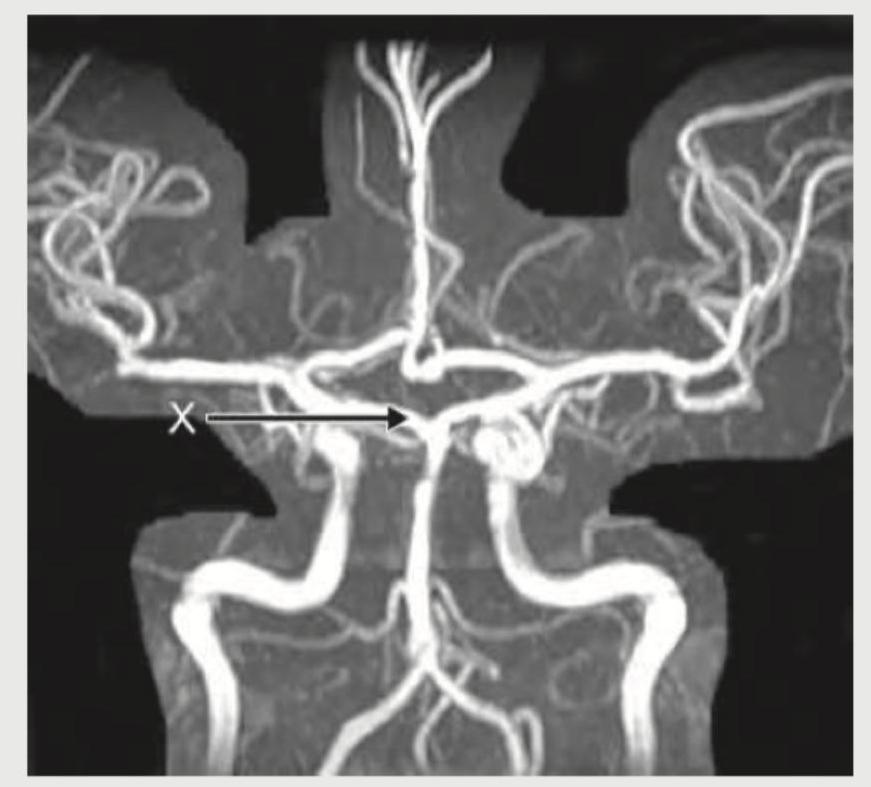
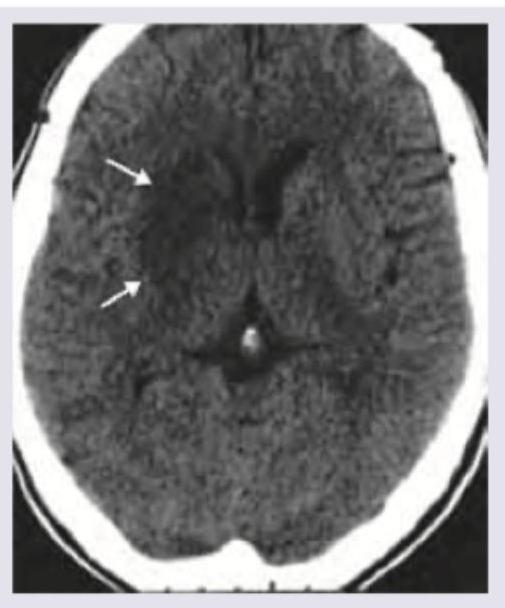
What is the name of the marked blood vessel shown in brain circulation?

Q52
What is the name of the marked blood vessel in the Circle of Willis?