All (368)Anatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
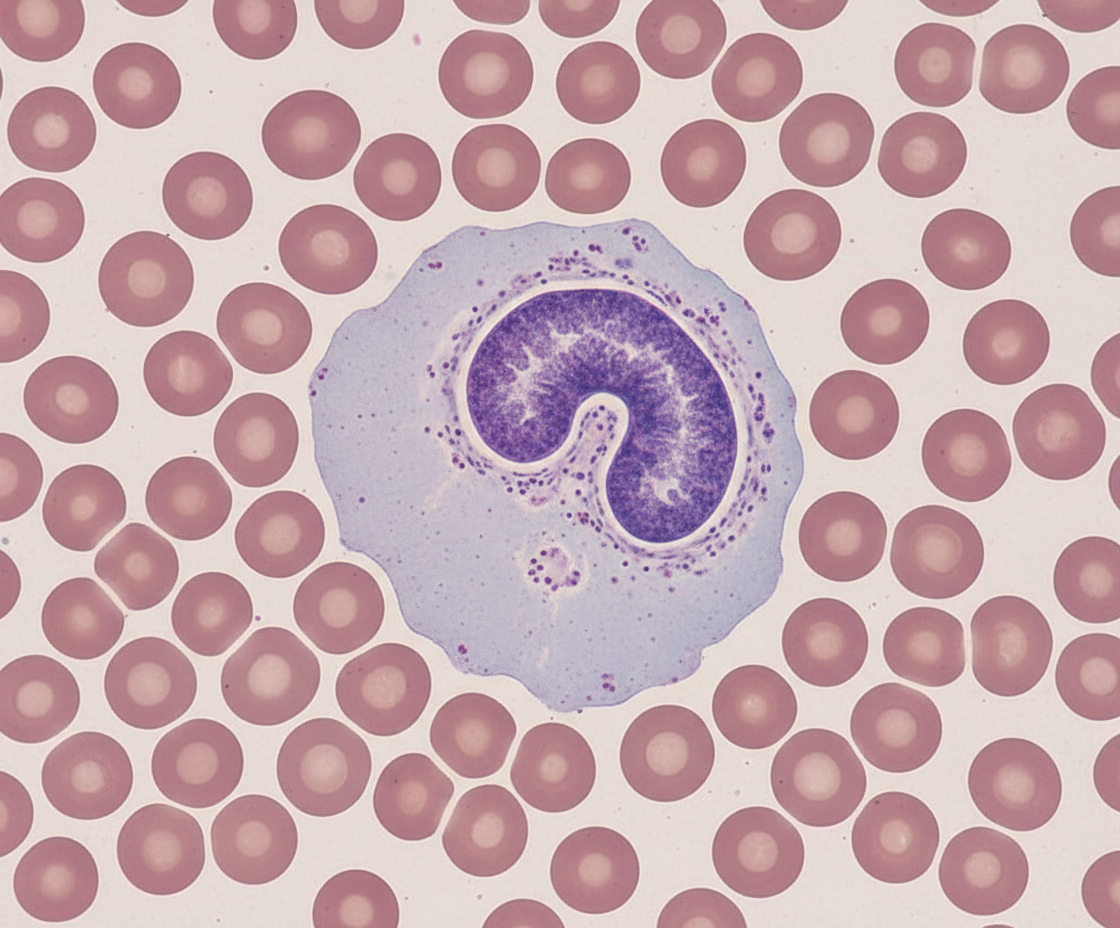
Q21
Identify the cell.
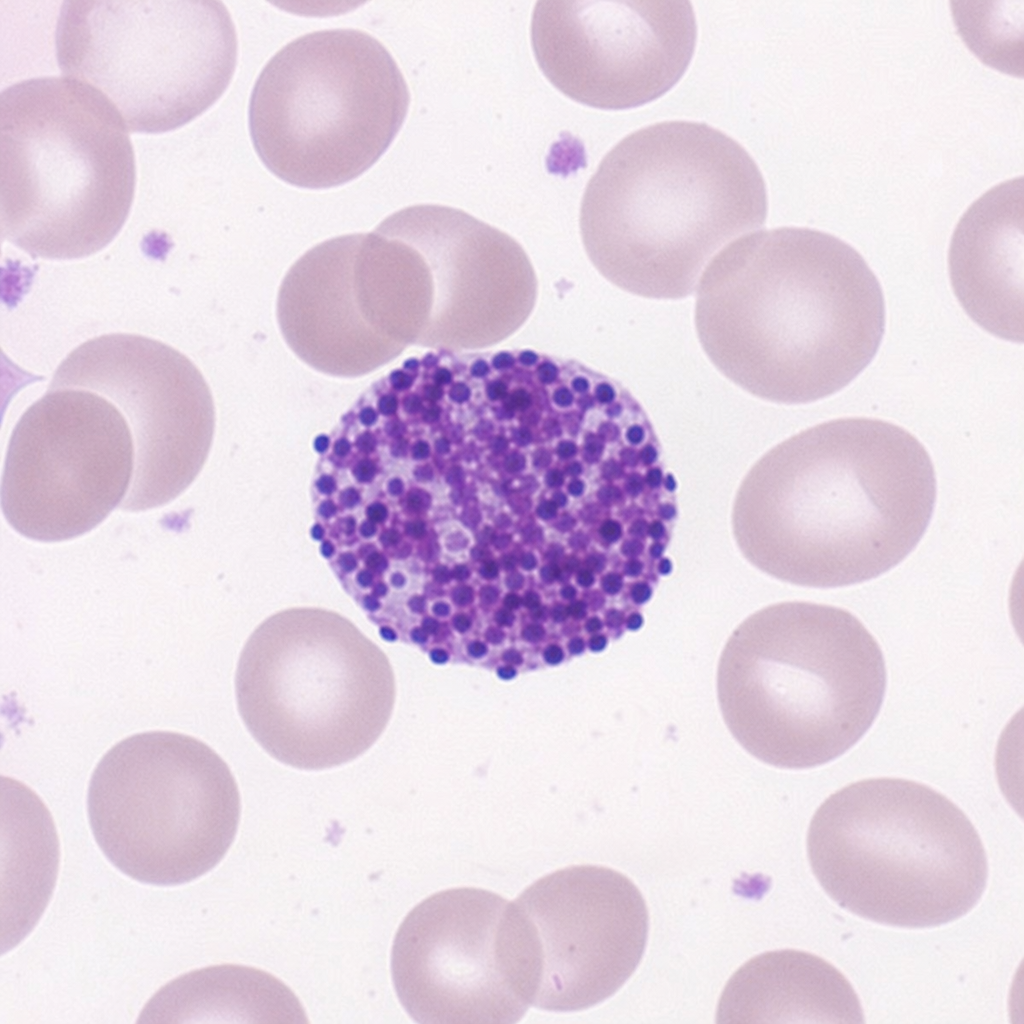
Q22
Identify the cell.
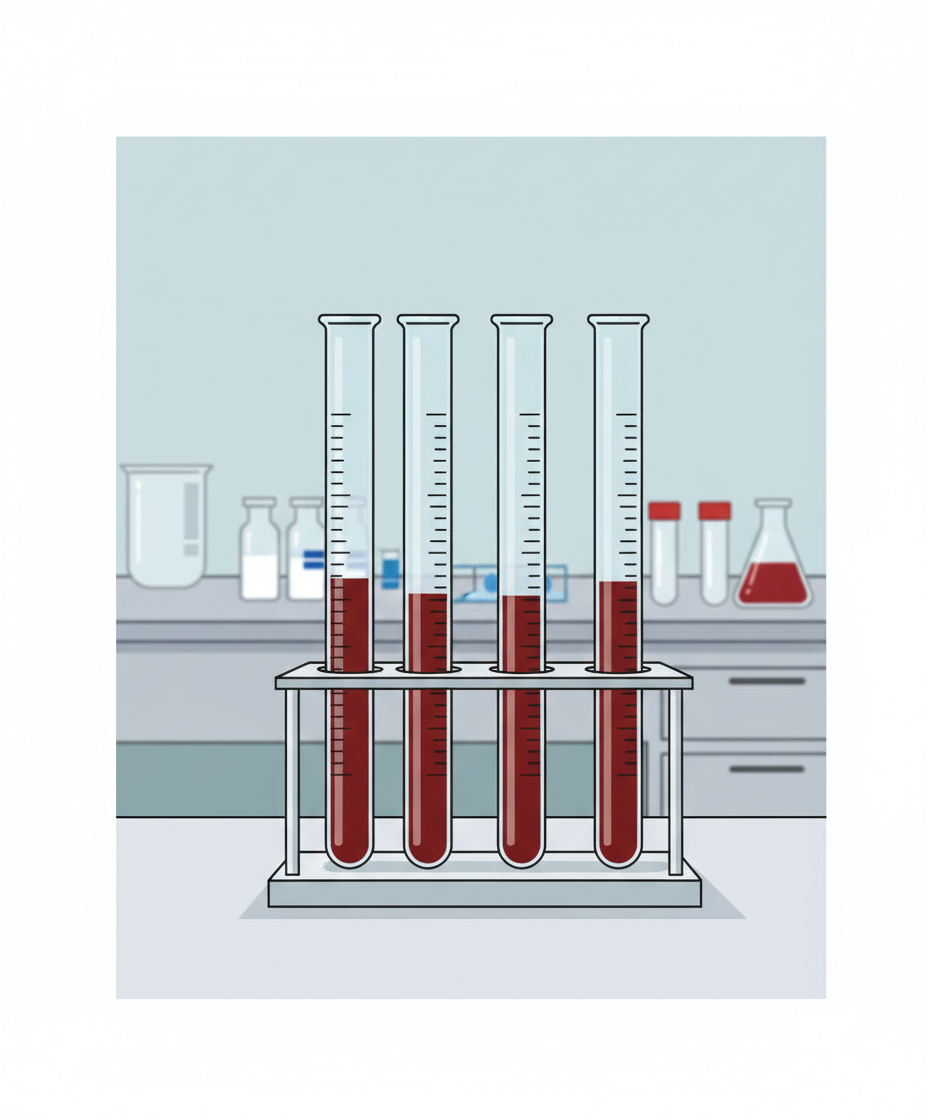
Q23
Name the test given.

Q24
Name the anticoagulant used in the following method.
Q25
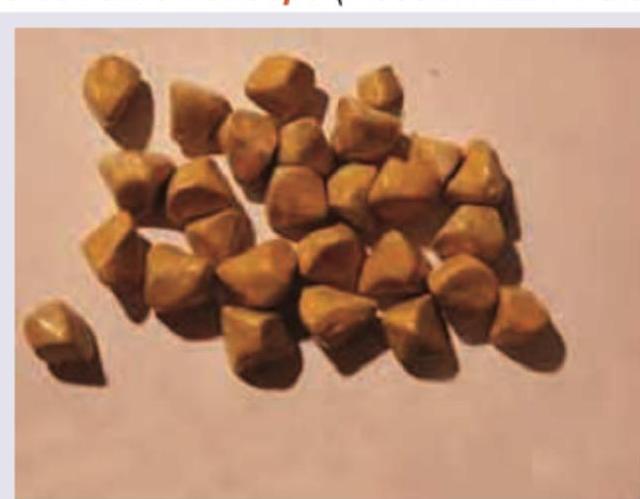
A 32-year-old male with a history of klebsiella infection presents with right upper quadrant pain and on performing cholecystectomy the following stones were seen. All the following statements are true regarding this condition except: (Recent NEET Pattern 2016-17)
Q26
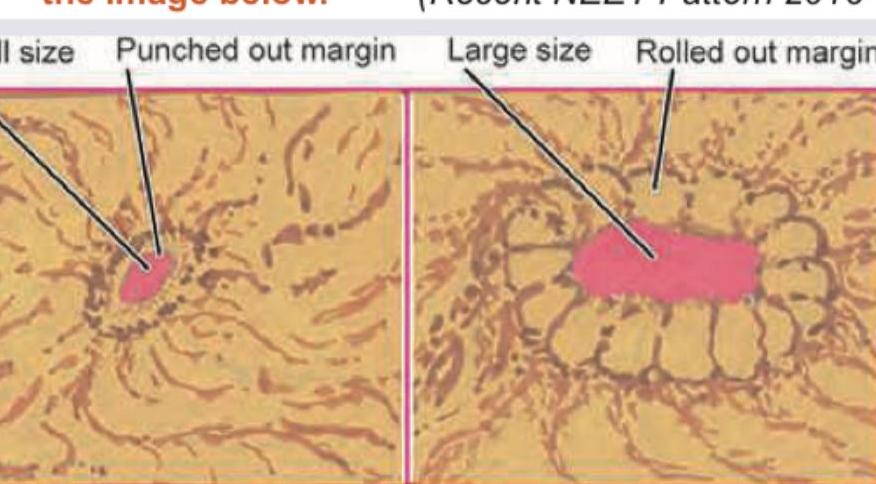
Identify the types of gastric ulcers labeled A and B in the image below.
Q27
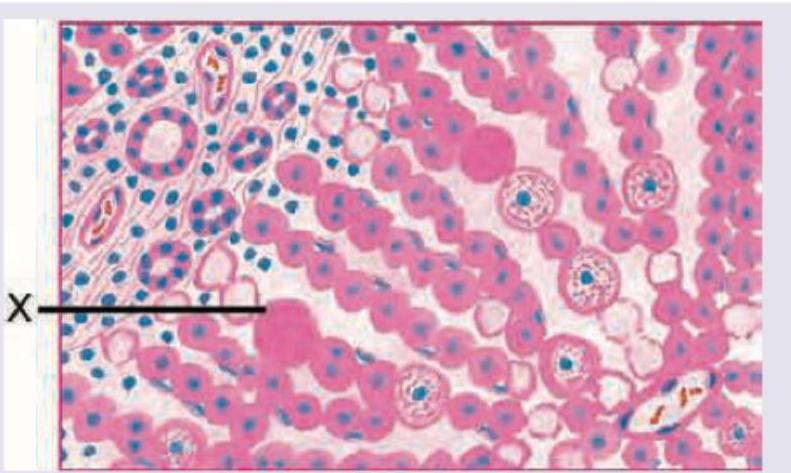
A 20-year-old college student presents with 7 day history of nausea and feeling feverish. He has tenderness in right upper quadrant and admits to high risk sexual behavior. The liver biopsy marking $X$ shows:
Q28
The resected specimen of a kidney is seen below. What is the diagnosis?

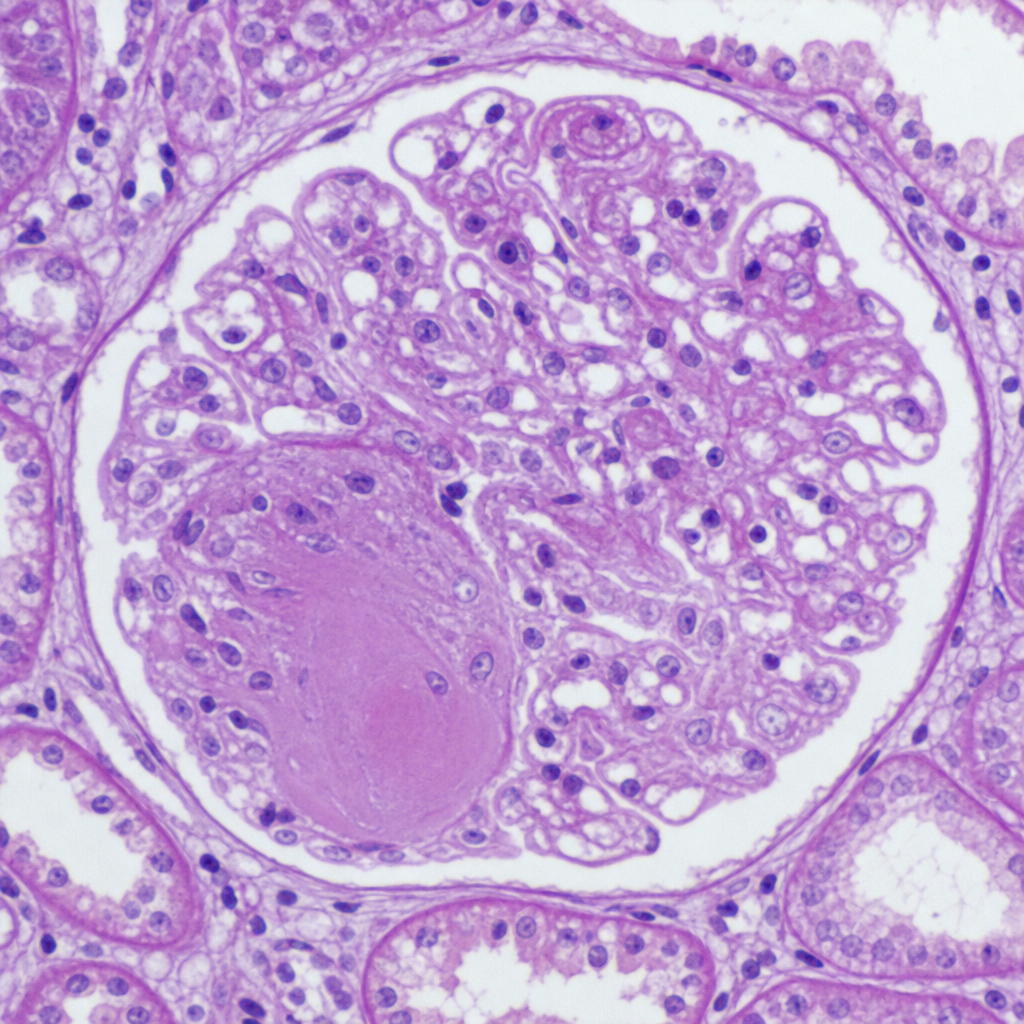
Q29
Identify the lesion shown in kidney biopsy of 6-year-old child with recurrent U.T.I and vesico-ureteric reflux.