All (368)Anatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q271
Identify the programme depicted by symbol as given in the image:

Q272
Act pertaining to symbol shown in the image given below was enacted in: (Recent NEET Pattern 2016-17)

Q273
Chairman of agency shown in the image given below:

Q274
Identify the organization depicted by the symbol in the image given below:
Q275
Identify the organization depicted by the symbol in the image given below:

Q276
Identify the organization depicted in the image given below:
Q277
Identify the organization depicted in the image given below:

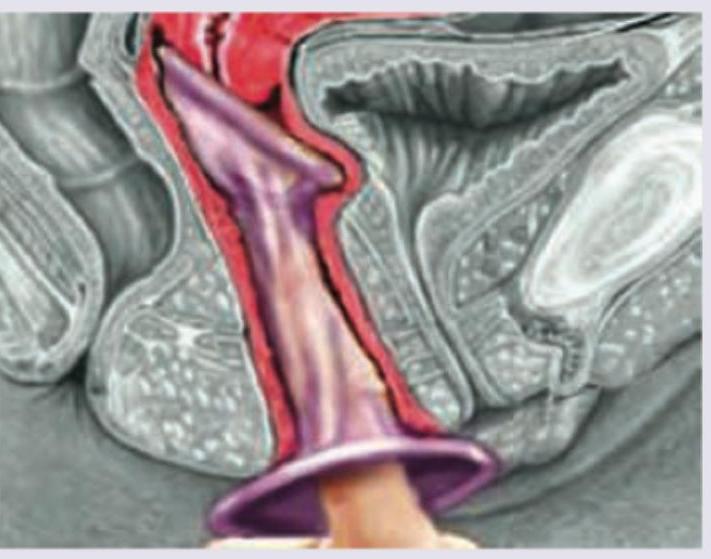
Q278
Which is not correct regarding the contraceptive method being used?