All (366)Anatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (16)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (10)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q201
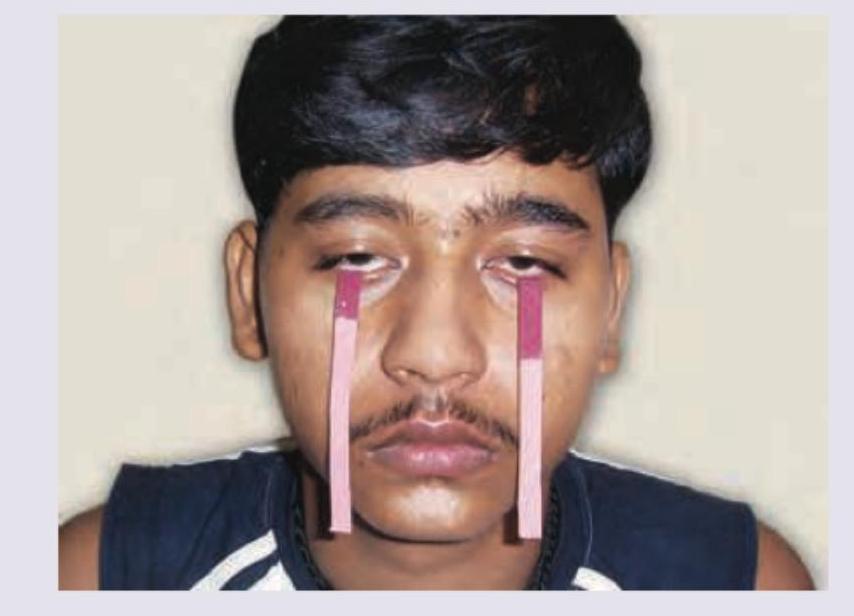
Which of the following test is being performed on the patient?

Q202
The test shown in the image is used for identifying a lesion in which cranial nerve?
Q203
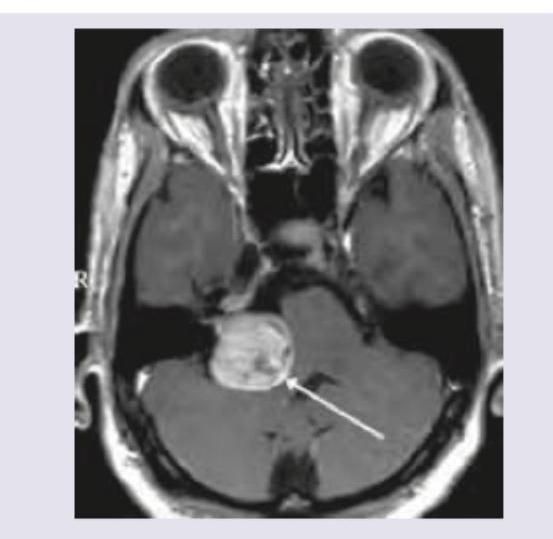
MRI Brain of a 40-year-old patient with progressive unilateral SNHL and tinnitus is shown below. Which is the most common extracanalicular nerve to be involved?
Q204
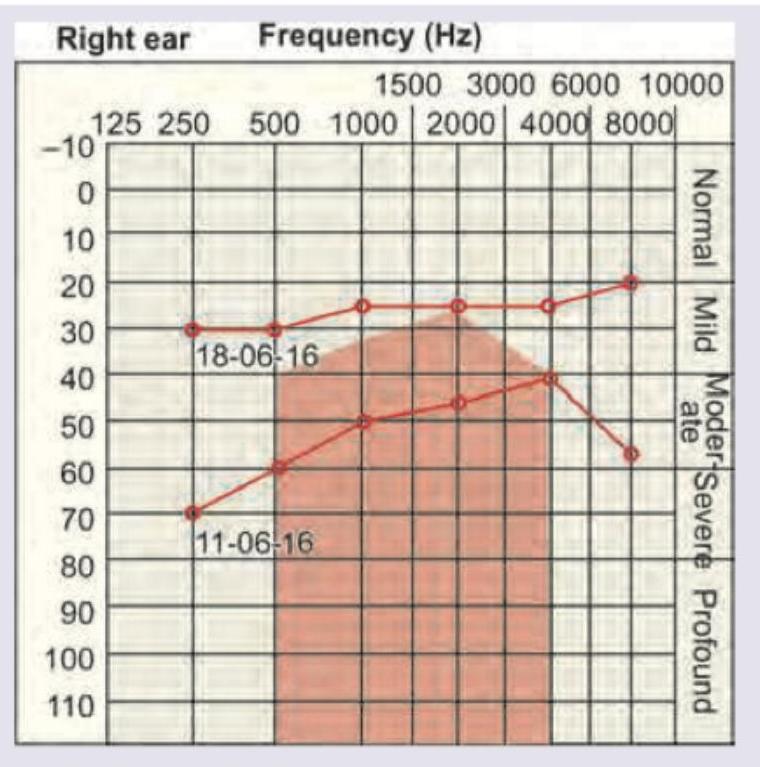
A 40-year-old woman presents with history of recurrent episodes of spinning sensation in horizontal direction with vertigo incapacitating her for hours and resolving with medication. She also report roaring tinnitus during the attacks. Her sequential audiogram done on 11.06.16 and 18.06.16 is given below. Diagnosis is:
Q205
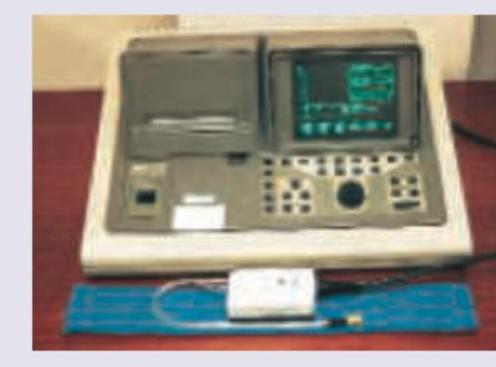
The instrument shown below is used in ENT for all except: (Recent NEET Pattern 2016-17)
Q206
Cosmetic reconstruction of this defect is best done at? (Recent NEET Pattern 2016-17)

Q207
All of the following statements regarding this instrument are true except: (Recent NEET Pattern 2016-17)

Q208
The facial features shown in the image are characteristic of:

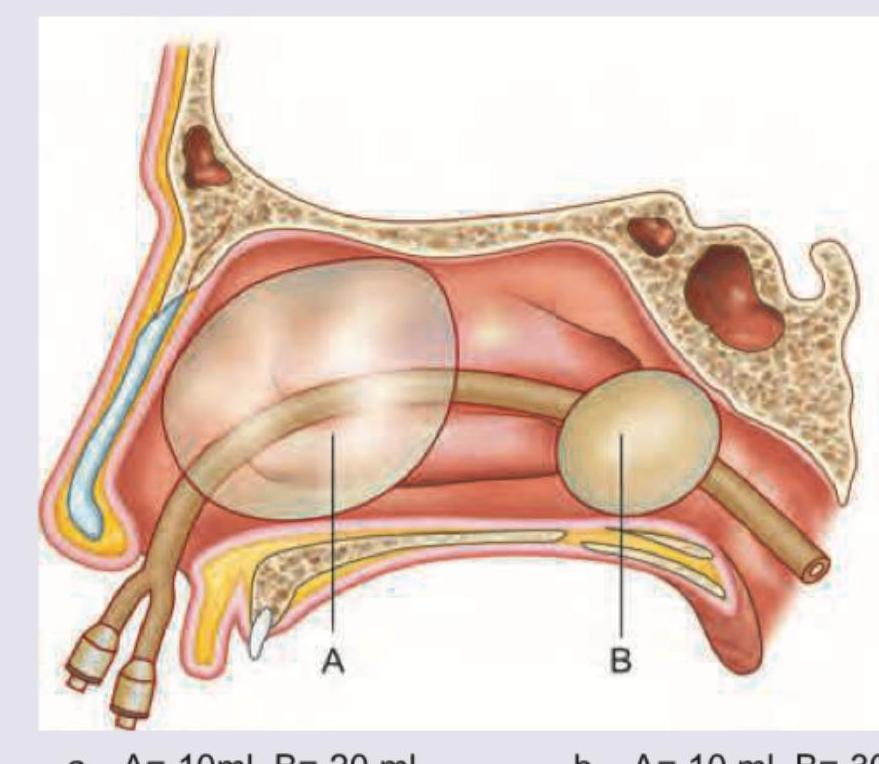
Q209
The volume of the balloons shown in epistaxis balloon is: (Recent NEET Pattern 2016-17)
Q210
The image shows which of the following tests being performed? (Recent NEET Pattern 2016-17)
