All (368)Anatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q11
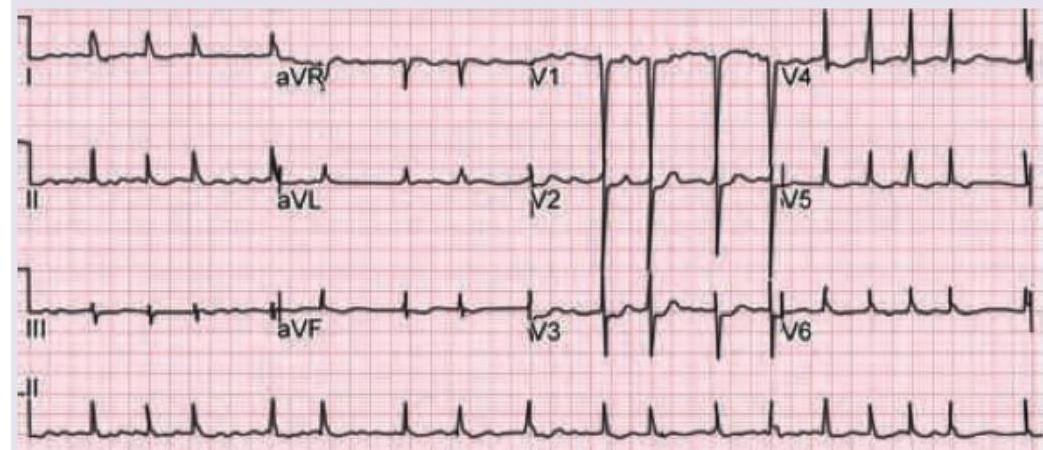
A 10-year-old child with Valvular heart disease on heart failure treatment, has the following ECG tracing. What is the diagnosis?
Q12
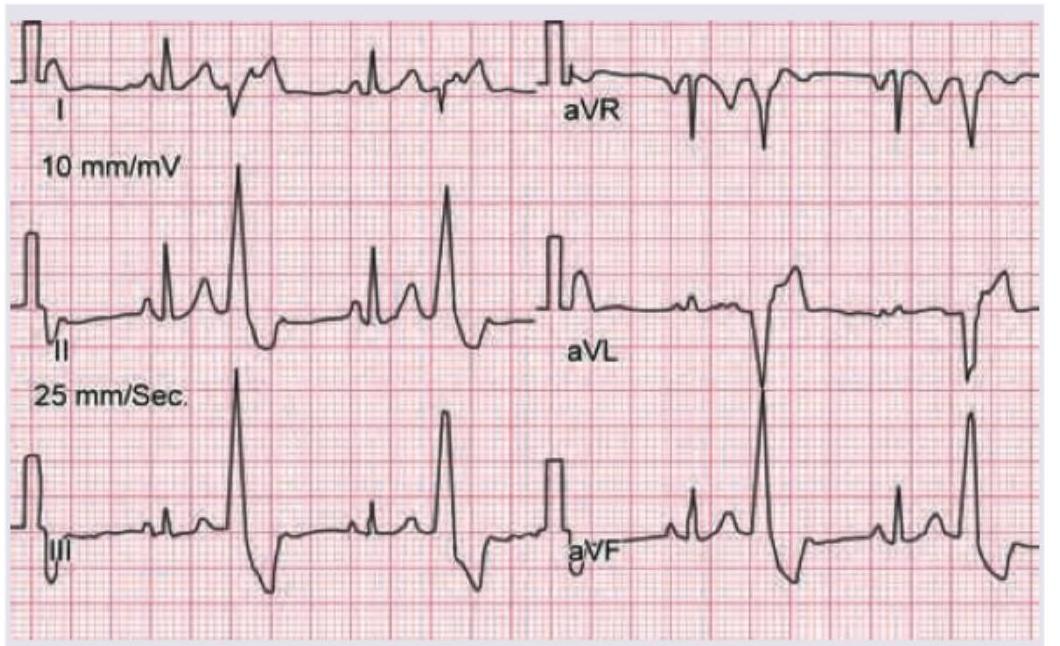
A 50-year-old woman with rheumatic heart disease is on medication for heart disease. She feels unwell for most part of the day. Which of the following medicine is responsible for the ECG changes shown below? (Recent NEET Pattern 2016-17)
Q13
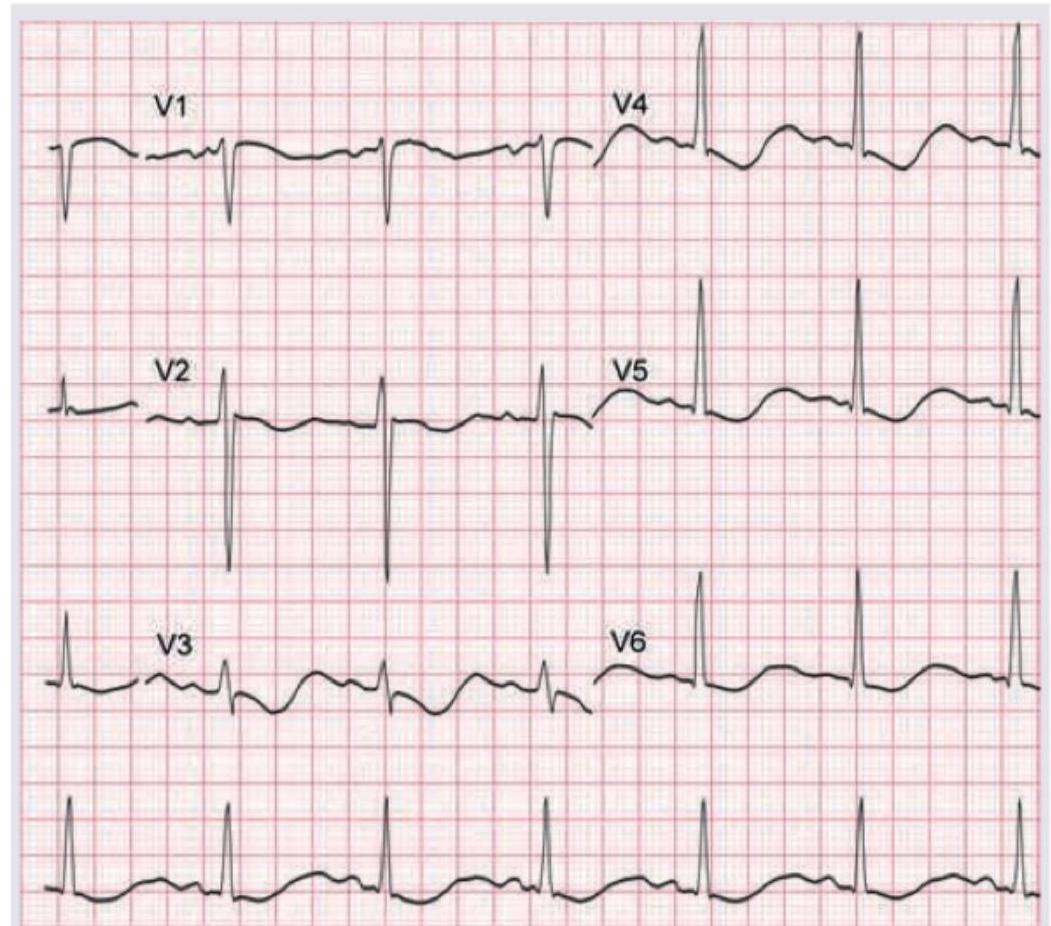
A 60-year-old hypertension patient presents with breathlessness. ECG was performed. What is the diagnosis? (Recent NEET Pattern 2016-17)
Q14
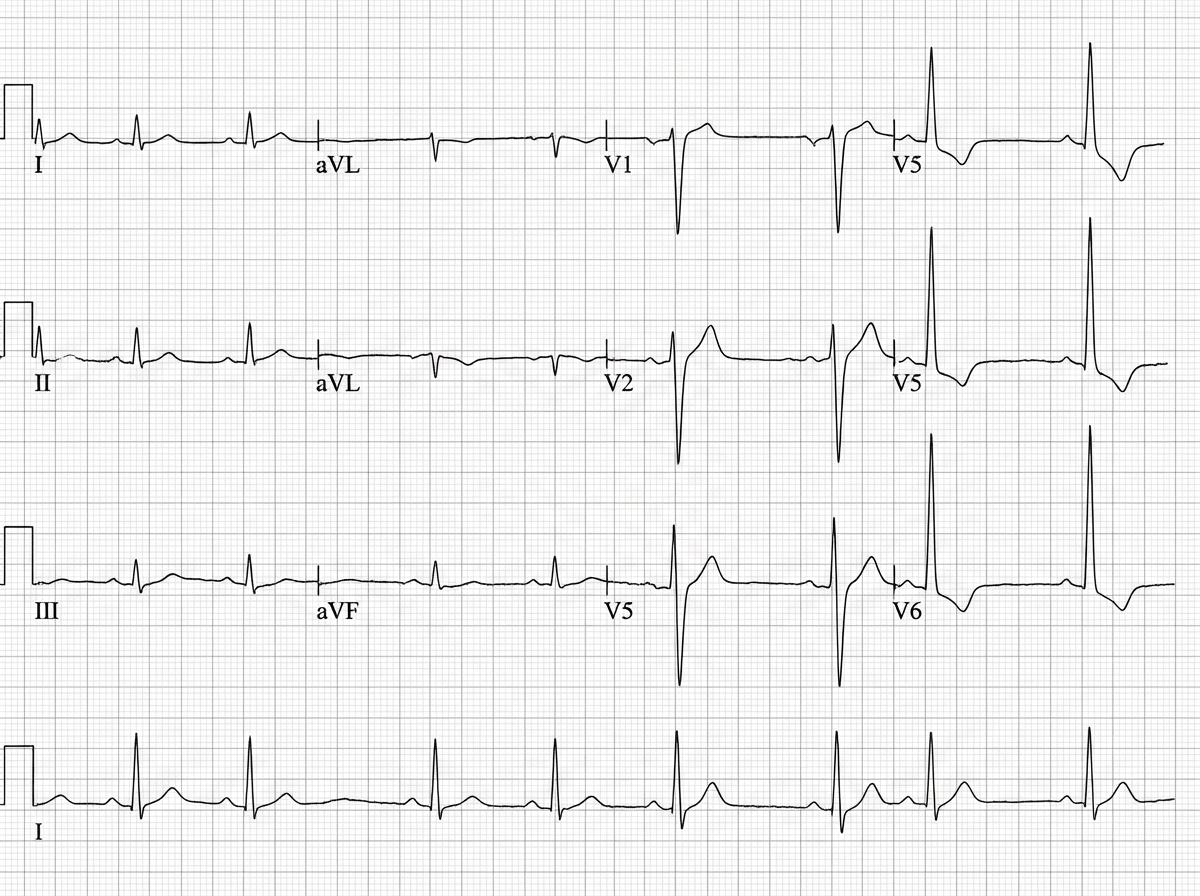
A 50-year-old smoker comes with complaints of ankle edema for last 3 months. The ECG shows all except: (Recent NEET Pattern 2016-17)
Q15
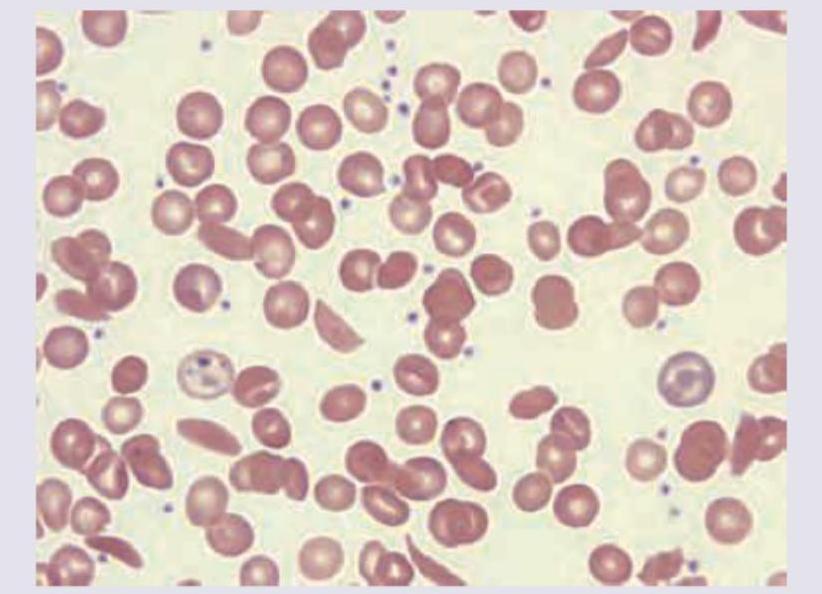
The patient with the following hematological abnormality presents with severe chest pain and difficulty in breathing. All are useful for managing this emergency except: