All (366)Anatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (16)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (10)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q141
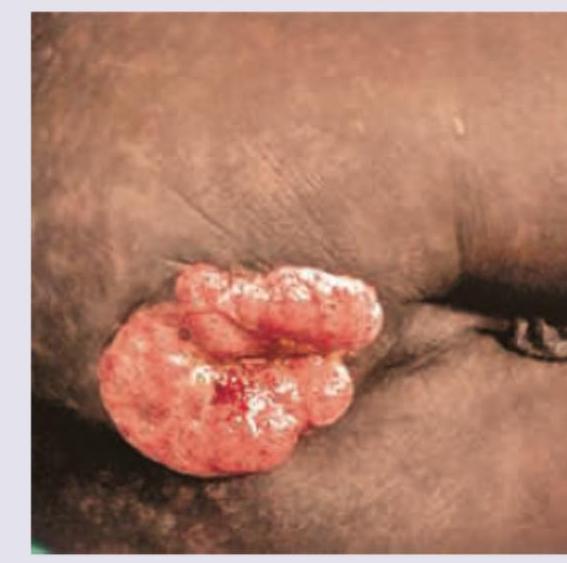
A 30-year-old AIDS patient presents with complaints as shown below. All are true about the condition except?