NEET-PG 2017 — Orthopaedics
11 Previous Year Questions with Answers & Explanations
What is correct about the fracture shown in the figure?

The given nature of injury will lead to the development of:
The contracture shown in the image is associated with all except:

The test performed below shows testing of which of the following nerve: (Recent NEET Pattern 2016-17)

Comment on the diagnosis based on examination findings shown below: (Recent NEET Pattern 2016-17)
All the following statements regarding this image are true except: (Recent NEET Pattern 2016-17)

What is the grade of fracture according to Garden's classification?

A sportsman presented to you after injury during practice exercise. You performed the test given in the image, and it came out as positive. What is the diagnosis?
Which of the following spine deformities is seen in the image?
Comment on the diagnosis of the presentation shown below:

NEET-PG 2017 - Orthopaedics NEET-PG Practice Questions and MCQs
Question 1: What is correct about the fracture shown in the figure?
- A. A= Bennett fracture, B= Rolando fracture (Correct Answer)
- B. A= Rolando fracture, B= Bennett fracture
- C. A= Boxer's fracture, B= Bennett fracture
- D. A= Bennett fracture, B= Boxer's fracture
Explanation: ***A= Bennett fracture, B= Rolando fracture*** * **Bennett fracture** (A) is an **intra-articular fracture** of the base of the first metacarpal bone with a characteristic **two-part fracture** pattern. It involves a small fragment of the metacarpal base remaining attached to the carpometacarpal joint, while the rest of the metacarpal is dislocated. * **Rolando fracture** (B) is a **comminuted intra-articular fracture** at the base of the first metacarpal. It is characterized by a **Y or T-shaped fracture pattern**, indicating a more complex, three-part or more fragment involvement compared to a Bennett fracture. *A= Rolando fracture, B= Bennett fracture* * This option incorrectly identifies A as a Rolando fracture; Image A clearly shows a **two-part fracture** typical of a Bennett fracture, not the comminuted pattern of a Rolando. * Similarly, B is incorrectly identified as a Bennett fracture as it depicts a **multi-fragmented, Y-shaped fracture**, which defines a Rolando fracture. *A= Boxer's fracture, B= Bennett fracture* * **Boxer's fracture** is a fracture of the **neck of the fifth metacarpal**, which is not depicted in either image A or B. Both images show fractures at the base of the first metacarpal. * Image A is a **Bennett fracture**, not a Boxer's fracture, and B is a **Rolando fracture**, not a Bennett fracture. *A= Bennett fracture, B= Boxer's fracture* * While A is correctly identified as a **Bennett fracture**, B is incorrectly identified as a Boxer's fracture. * As previously stated, a **Boxer's fracture affects the fifth metacarpal**, whereas image B clearly shows a fracture of the first metacarpal base with multiple fragments.
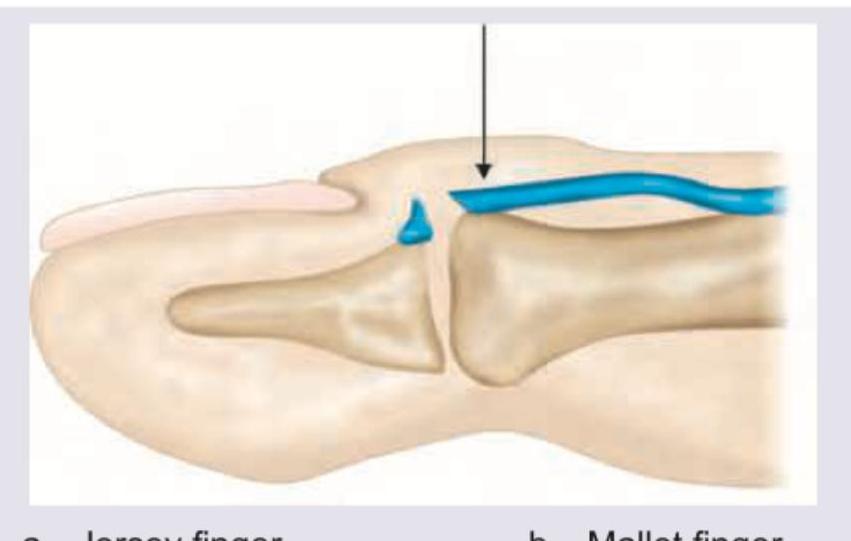
Question 2: The given nature of injury will lead to the development of:
- A. Jersey finger
- B. Mallet finger (Correct Answer)
- C. Jammed finger
- D. Boxer knuckle
Explanation: ***Mallet finger*** - The image shows a **rupture of the extensor tendon** at its insertion into the distal phalanx, or an avulsion fracture of the distal phalanx, causing an inability to extend the distal interphalangeal (DIP) joint. - This injury results in the characteristic **flexion deformity** of the DIP joint, known as mallet finger. *Jersey finger* - This injury involves the **rupture of the flexor digitorum profundus tendon** from its insertion at the base of the distal phalanx. - Patients cannot actively **flex their DIP joint**, unlike the extensor tendon injury shown. *Jammed finger* - This is a general term for an **axial load injury** to the finger, usually causing a sprain or mild fracture without a specific tendon rupture as depicted. - It typically results from impact on the fingertip, leading to **ligamentous injury** or joint capsule damage. *Boxer knuckle* - **Boxer's knuckle** refers to a sagital band rupture at the metacarpophalangeal (MCP) joint, affecting the central slip of the extensor tendon. - This injury primarily involves the **MCP joint** and not the DIP joint, as shown in the image.
Question 3: The contracture shown in the image is associated with all except:
- A. Seen in cirrhosis
- B. Involves the ring and little finger
- C. Table top test is negative (Correct Answer)
- D. Clostridial collagenase for resolution
Explanation: ***Table top test is negative*** - The image shows a hand affected by **Dupuytren's contracture**, characterized by fixed flexion deformities of the finger joints. - In Dupuytren's contracture, the **tabletop test** is typically **positive** (meaning the hand cannot be laid flat on a table) when the metacarpophalangeal (MCP) or proximal interphalangeal (PIP) joint contracture exceeds 30 degrees, indicating significant fascial thickening and shortening. *Seen in cirrhosis* - **Dupuytren's contracture** is indeed associated with conditions like **alcoholism** and **liver cirrhosis**, though the exact pathophysiological link is not fully understood. - Other associated conditions include diabetes mellitus, manual labor, and certain anti-epileptic medications. *Involves the ring and little finger* - Dupuytren's contracture most commonly affects the **ulnar side of the hand**, particularly the **ring finger** and **little finger**, due to fibrosis and shortening of the palmar fascia. - It can also involve the middle finger and rarely the index finger and thumb. *Clostridial collagenase for resolution* - **Collagenase clostridium histolyticum (CCH)**, derived from *Clostridium histolyticum*, is an approved non-surgical treatment for Dupuytren's contracture. - It works by injecting the enzyme directly into the palmar cord to **dissolve the collagen fibers** responsible for the contracture, allowing for manipulation to release the contracture.
Question 4: The test performed below shows testing of which of the following nerve: (Recent NEET Pattern 2016-17)
- A. Median nerve
- B. Ulnar nerve (Correct Answer)
- C. Radial nerve
- D. Axillary nerve
Explanation: ***Ulnar nerve*** - The image shows a patient with inability to adequately flex the **ring and little fingers**, a classic sign of **ulnar nerve palsy**. This is known as the **"ulnar claw"** when the patient attempts to make a fist or extend the fingers. - The ulnar nerve innervates most of the **intrinsic hand muscles**, including the **interossei** and the **medial two lumbricals (ring and little fingers)**, which are responsible for flexion at the metacarpophalangeal joints and extension at the interphalangeal joints of these digits. *Median nerve* - **Median nerve injury** typically results in inability to **oppose the thumb** (ape hand deformity) and sensory loss over the radial three and a half digits. - It affects the **flexor muscles of the forearm** and the **thenar muscles**, not primarily the ring and little finger flexion shown. *Radial nerve* - **Radial nerve injury** causes **wrist drop** and **finger drop** due to paralysis of the extensors of the wrist and fingers. - It primarily affects **extension** of the wrist and fingers, rather than the intrinsic hand function of flexion shown in the image. *Axillary nerve* - The **axillary nerve** primarily innervates the **deltoid muscle** and **teres minor**, responsible for shoulder abduction and external rotation. - Injury to the axillary nerve would result in **shoulder weakness** and sensory loss over the lateral shoulder, with no direct impact on hand or finger function.
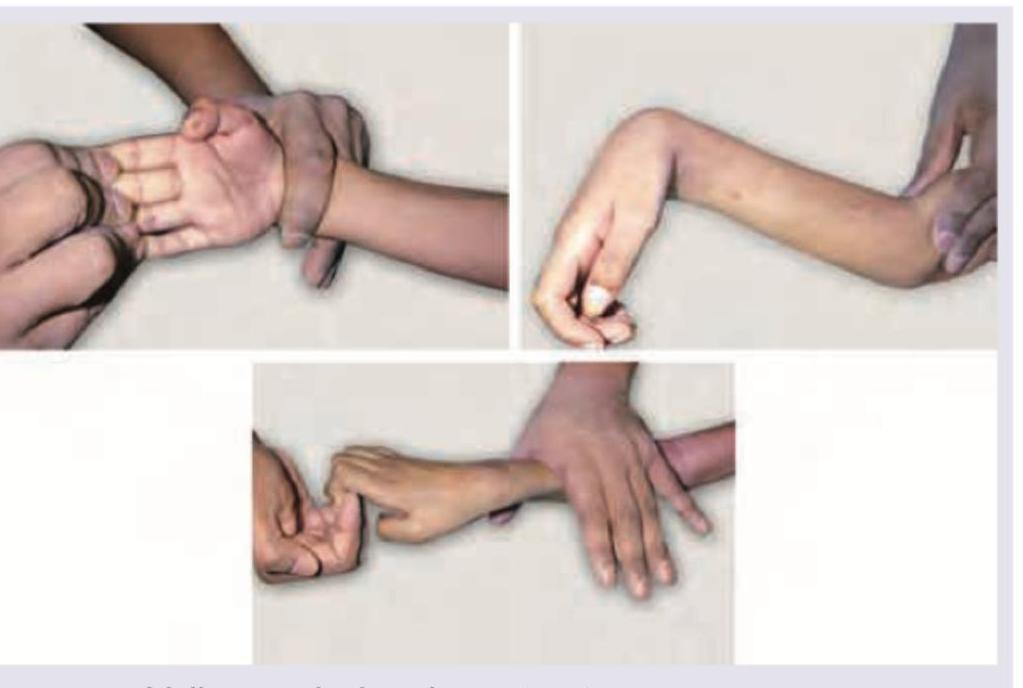
Question 5: Comment on the diagnosis based on examination findings shown below: (Recent NEET Pattern 2016-17)
- A. Volkmann ischemic contracture (Correct Answer)
- B. Ulnar tunnel syndrome
- C. Cubital tunnel syndrome
- D. Wartenberg's syndrome
Explanation: ***Volkmann ischemic contracture*** - The images show a **fixed flexion deformity of the wrist and fingers**, along with **forearm pronation**, which is characteristic of Volkmann's ischemic contracture. - This condition results from **ischemia to the forearm muscles**, leading to muscle necrosis and subsequent fibrosis and contracture. *Ulnar tunnel syndrome* - This syndrome involves compression of the **ulnar nerve** at the wrist. - Symptoms typically include **numbness and tingling in the ring and little fingers**, and hand weakness, which are not depicted as the primary finding here. *Cubital tunnel syndrome* - This condition involves compression of the **ulnar nerve** at the elbow. - It presents with similar sensory and motor deficits to ulnar tunnel syndrome but specifically related to the elbow, not the characteristic fixed deformity shown. *Wartenberg's syndrome* - Also known as **superficial radial nerve entrapment**, it involves compression of the superficial branch of the radial nerve. - This typically causes **sensory symptoms** (pain, numbness, paresthesia) on the back of the hand and thumb, without the gross motor contracture seen in the images.
Question 6: All the following statements regarding this image are true except: (Recent NEET Pattern 2016-17)
- A. This condition could result from student's elbow
- B. It is secondary to trauma
- C. This is a soft tissue tumor (Correct Answer)
- D. This condition is due to inflammation of the sub-cutaneous fat
Explanation: ***This is a soft tissue tumor*** - The image shows a swelling over the olecranon process, which is characteristic of **olecranon bursitis**. This condition is an **inflammation of the bursa**, not a soft tissue tumor. - A tumor implies an abnormal growth of tissue that can be benign or malignant, which is not depicted here; the swelling is related to fluid accumulation within a bursa. *This condition could result from student's elbow* - **Student's elbow** is another name for olecranon bursitis, which is the condition depicted in the image. - This common term refers to the inflammation of the olecranon bursa, often caused by **repetitive pressure or trauma** to the elbow, such as leaning on it for extended periods while studying. *It is secondary to trauma* - **Trauma**, especially repetitive minor trauma or a single significant impact, is a very common cause of olecranon bursitis due to injury to the bursa. - This trauma can lead to inflammation and fluid accumulation within the bursa, causing the characteristic swelling. *This condition is due to inflammation of the sub-cutaneous fat* - The condition shown is **olecranon bursitis**, which is an inflammation of the **olecranon bursa**. - The olecranon bursa is a fluid-filled sac that lies between the skin and the olecranon process of the ulna to reduce friction, and its inflammation is distinct from inflammation of the subcutaneous fat (panniculitis).
Question 7: What is the grade of fracture according to Garden's classification?
- A. Grade I
- B. Grade II
- C. Grade III (Correct Answer)
- D. Grade IV
Explanation: ***Grade III*** - This image shows a **complete displaced fracture** of the femoral neck, but with the **distal fragment in valgus** position, which corresponds to Garden Grade III. - In Garden Grade III, the fracture is **complete and displaced**, but there is still some **engagement** of the fracture surfaces, leading to the valgus alignment of the head on the shaft. *Grade I* - Garden Grade I refers to an **incomplete impacted valgus fracture** of the femoral neck. - The fracture line is visible, but there is no displacement, and the head is tilted into a valgus position relative to the neck. *Grade II* - Garden Grade II describes a **complete but non-displaced fracture** of the femoral neck. - The fracture line extends across the entire neck, but the fragments remain in anatomical alignment without angulation or displacement. *Grade IV* - Garden Grade IV is characterized by a **complete and fully displaced fracture** of the femoral neck, with the **femoral head completely separated** from the shaft and in a neutral or varus position. - There is a complete loss of contact and alignment between the femoral head and the shaft, indicating significant instability.
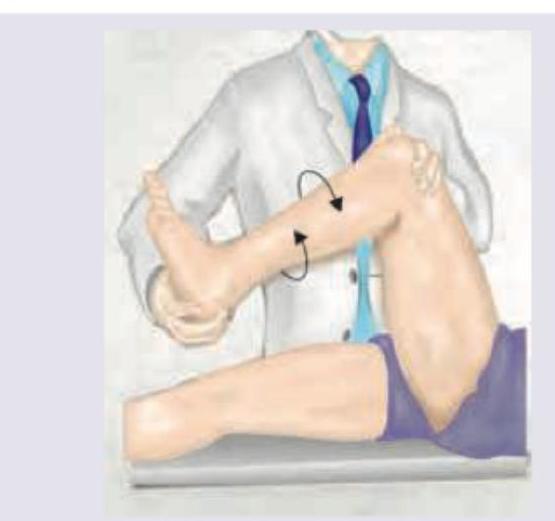
Question 8: A sportsman presented to you after injury during practice exercise. You performed the test given in the image, and it came out as positive. What is the diagnosis?
- A. Anterior cruciate ligament tear (Correct Answer)
- B. Posterior cruciate ligament tear
- C. Medial meniscus tear
- D. Medial collateral ligament tear
Explanation: ***Anterior cruciate ligament tear*** - The image depicts the **Lachman test**, a highly sensitive and specific clinical test for **ACL integrity**. - A positive Lachman test, characterized by *increased anterior tibial translation* and a *soft or absent endpoint*, confirms an **ACL tear**. *Posterior cruciate ligament tear* - A PCL tear is identified by tests like the **posterior drawer test** or **posterior sag sign**, which show *posterior tibial translation*. - The test shown in the image specifically assesses **anterior stability**, not posterior. *Medial meniscus tear* - Medial meniscus tears are typically diagnosed with tests like **McMurray's test** or **Apley's grind test**, which involve *rotation* and *compression* of the knee. - While a crucial knee structure, the meniscus does not primarily contribute to **anterior-posterior stability** in the way the ACL does. *Medial collateral ligament tear* - An MCL tear is detected by applying a **valgus stress** to the knee at various degrees of flexion. - This tear presents with *medial joint line pain* and *instability to valgus stress*, which is not assessed by the depicted test.
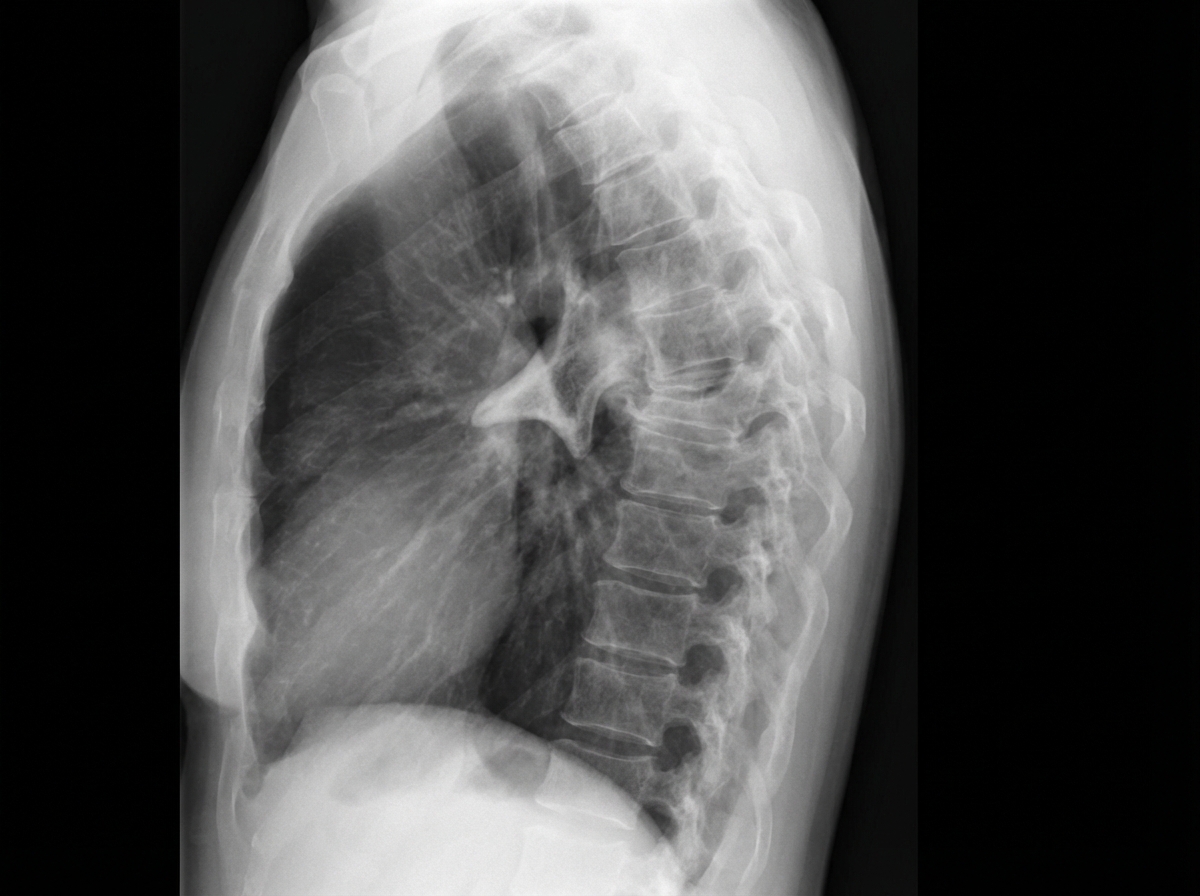
Question 9: Which of the following spine deformities is seen in the image?
- A. Kyphosis
- B. Gibbus (Correct Answer)
- C. Lordosis
- D. Scoliosis
Explanation: ***Gibbus*** - A **gibbus deformity** is a sharply angular posterior projection of a vertebral segment, caused by the collapse of one or more vertebral bodies. - Most commonly due to **Pott's disease (spinal tuberculosis)**, where vertebral body destruction leads to a focal, acute-angle hump. - The image clearly shows a **localized, sharp posterior angulation** in the thoracic spine, which is characteristic of a gibbus. *Kyphosis* - **Kyphosis** refers to an exaggerated **posterior curvature** of the thoracic spine, producing a "rounded back." - While a gibbus is technically a severe form of kyphosis, kyphosis alone describes a more **generalized, smooth curve** — not the focal, angular hump seen in the image. *Lordosis* - **Lordosis** describes an **anterior (forward) curvature** of the lumbar spine, often called "swayback." - This is not seen in the image, which displays a prominent **posterior** projection, not an anterior one. *Scoliosis* - **Scoliosis** is a **lateral (side-to-side) curvature** of the spine, seen as a deviation when viewed from behind. - The image shows a deformity in the **sagittal plane** (anterior-posterior), not the coronal plane, ruling out scoliosis.
Question 10: Comment on the diagnosis of the presentation shown below:
- A. Unicameral bone cyst (Correct Answer)
- B. Aneurysmal bone cyst
- C. Osteoblastoma
- D. Osteoclastoma
Explanation: ***Unicameral bone cyst*** - This X-ray shows a **well-defined, lytic lesion** in the proximal humerus, consistent with a unicameral bone cyst, often presenting in the **metaphysis** of long bones in children and adolescents. - The lesion has a **thin, sclerotic rim** and shows **no significant periosteal reaction** or soft tissue mass, which are classic features. *Aneurysmal bone cyst* - While also a lytic lesion, an aneurysmal bone cyst typically appears more **expansile** and **multiloculated**, often with a **"soap bubble" appearance**. - It usually has a **thicker, more irregular rim** and can present with faster growth or more aggressive features than a unicameral bone cyst. *Osteoblastoma* - Osteoblastomas are typically **osteoblastic (bone-forming)** tumors, which would appear more **sclerotic** or mixed lytic-sclerotic on X-ray, rather than a purely lytic lesion like the one shown. - They commonly affect the **spine or long bones**, but their radiographic appearance of predominant bone formation is not seen here. *Osteoclastoma* - Osteoclastomas, also known as **giant cell tumors of bone**, are usually found in the **epiphysis** of long bones in mature skeletons, which is a different location than observed. - They are typically **aggressive lytic lesions** with poorly defined margins and can extend to the articular surface, which is not characteristic of the well-demarcated lesion in the image.