NEET-PG 2017 — Ophthalmology
16 Previous Year Questions with Answers & Explanations
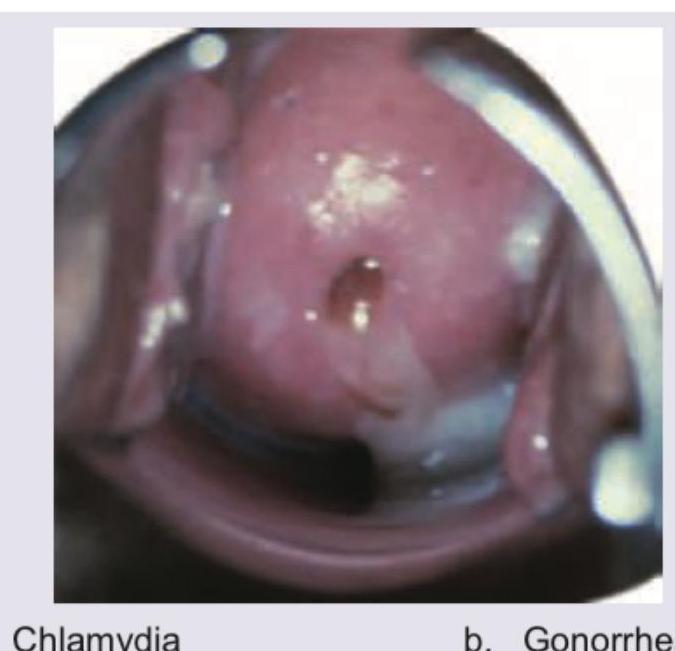
Identify the STD. (Recent Neet Pattern 2016-17)
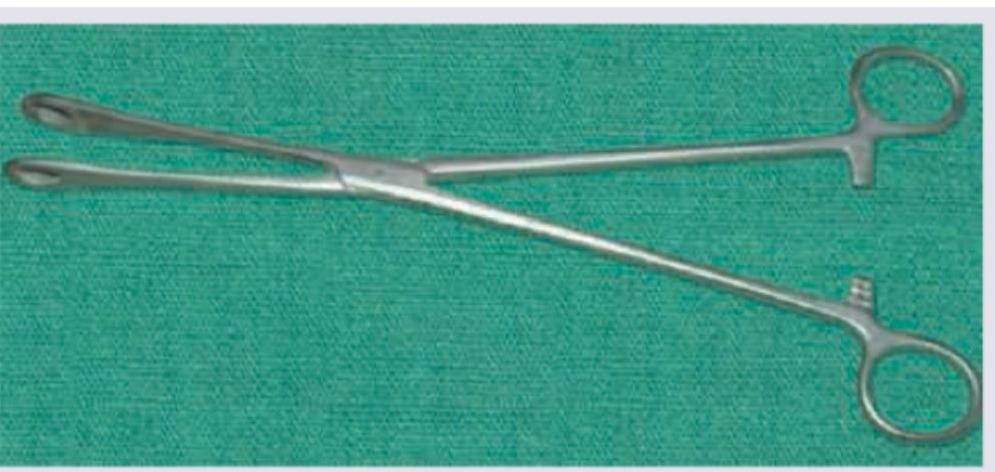
Identify the instrument:
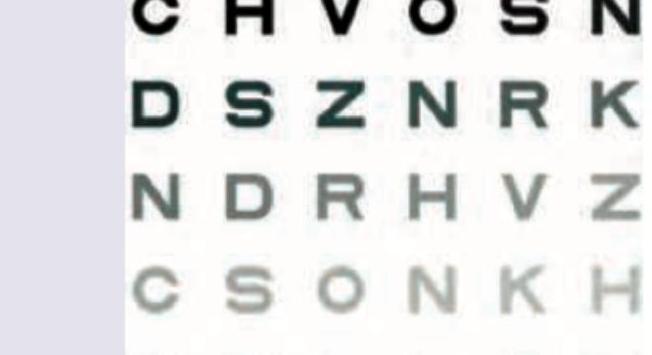
The following alphabet of Snellen's chart will subtend an angle of how many minutes at nodal point of the eye?

The chart shown in the image is:
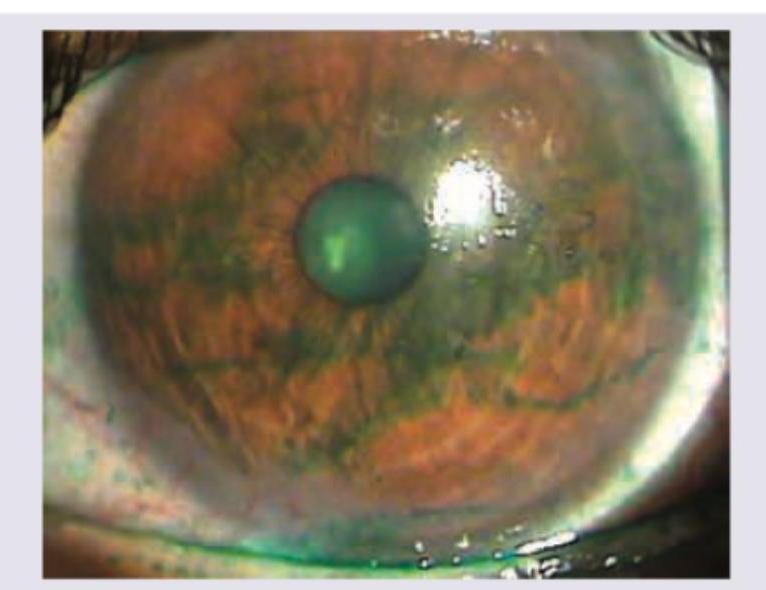
Identify the stain instilled in the eye in the following image:
A patient from slum presents with grittiness in eyes. Everted eyelid shows: (Recent NEET Pattern 2016-17)

All are causes of the presentation shown below except:
A 30-year-old school teacher presents with complaints of red eye with photophobia. Ocular findings are shown below. All are true about the condition shown except: (Recent NEET Pattern 2016-17)
The given FFA appearance occurs due to accumulation of dye in which of the following layers of retina?
A 75-year-old Englishman living in India presents to OPD with complaints of gradual onset painless, progressive blurring of central vision. He says he could earlier drive to the hospital by himself but is not able to do so now. Slit lamp examination is normal. Fundus examination is given below. What is the diagnosis?
NEET-PG 2017 - Ophthalmology NEET-PG Practice Questions and MCQs
Question 1: Identify the STD. (Recent Neet Pattern 2016-17)
- A. Chlamydia (Correct Answer)
- B. Gonorrhea
- C. Syphilis
- D. Chancroid
Explanation: ***Chlamydia*** - The image exhibits **cervicitis** with a visible **purulent exudate** and **cervical edema**, which is highly characteristic of **Chlamydia trachomatis** infection. - Given that Chlamydia is often **asymptomatic** or presents with non-specific symptoms, direct visualization of such changes on the cervix is a key diagnostic indicator in symptomatic cases. *Gonorrhea* - While gonorrhea can also cause cervicitis with purulent discharge, the specific appearance in the image with more pronounced **edema** and somewhat **friable cervix** is more classically associated with Chlamydia in many clinical presentations. - Differentiation often requires **laboratory testing** (e.g., NAAT) as visual signs can overlap, but the depicted features lean more towards Chlamydia. *Syphilis* - Syphilis is typically characterized by **chancres** (painless ulcers) in its primary stage, or rashes and condylomata lata in secondary syphilis, none of which are seen in this image. - The image shows inflammation and discharge, not ulcerative lesions. *Chancroid* - Chancroid is characterized by **painful genital ulcers** with a characteristic soft base and often associated with **buboes** (swollen lymph nodes). - The findings in the image—cervical inflammation and discharge—do not align with the typical presentation of chancroid.
Question 2: Identify the instrument:
- A. Sponge-holding forceps (Correct Answer)
- B. Ovum forceps
- C. Kocher forceps
- D. Allis forceps
Explanation: ***Sponge-holding forceps*** - This image clearly shows **sponge-holding forceps**, identifiable by their **long handles** and **fenestrated, serrated jaws** used for holding swabs or sponges during surgical procedures. - The jaws are designed to securely grip materials without crushing them, crucial for gentle tissue handling or applying antiseptics. *Ovum forceps* - **Ovum forceps** typically have **cup-shaped jaws** with or without teeth, specifically designed for removing placental fragments or uterine contents. - Their jaws are usually shorter and more rounded than those depicted. *Kocher forceps* - **Kocher forceps** are characterized by their **transverse serrations** and **1x2 teeth** at the tip, designed for strong and atraumatic grasping of tissue. - The jaws in the image are clearly fenestrated and do not have the characteristic teeth of Kocher forceps. *Allis forceps* - **Allis forceps** have **multiple fine teeth** at the tip that intermesh, providing a secure but potentially traumatic grip on tissue. - They are used for grasping and holding tissue that is to be removed, distinguishing them from the broader, fenestrated jaws shown.
Question 3: The following alphabet of Snellen's chart will subtend an angle of how many minutes at nodal point of the eye?
- A. 1
- B. 3
- C. 5 (Correct Answer)
- D. 10
Explanation: ***Correct Option: 5 minutes*** - The **entire optotype (letter)** of a Snellen's chart subtends an angle of **5 minutes of arc** at the nodal point of the eye when viewed from the standard testing distance - This is the fundamental design principle of the Snellen chart for visual acuity testing - At 6 meters (20 feet), a letter on the 6/6 (20/20) line subtends 5 minutes of arc in total height and width - This standardization allows for consistent visual acuity measurement across different testing scenarios *Incorrect: 1 minute* - This is the angle subtended by **each component part** of the letter (e.g., the width of a stroke or gap between strokes) - Not the angle for the entire letter - Used to define the detail that must be resolved for normal vision *Incorrect: 3 minutes* - No standard optical principle supports this value - Not related to Snellen chart design parameters *Incorrect: 10 minutes* - This angle is too large for standard Snellen chart optotypes - Would indicate significantly reduced visual acuity requirements - Not consistent with 6/6 (20/20) vision standards
Question 4: The chart shown in the image is:
- A. Ishihara's chart
- B. Snellen's chart (Correct Answer)
- C. Farnsworth-Munsell hue test
- D. Pelli-Robson chart
Explanation: ***Snellen's chart*** - The image displays a series of rows with **optotypes (letters)** that decrease in size, which is characteristic of a **Snellen chart**. - This chart is specifically used to measure **visual acuity** by determining the smallest row of letters a person can read at a specific distance. *Ishihara's chart* - **Ishihara charts** are used to test for **color blindness** and consist of plates with colored dots that form numbers or patterns, which are not depicted in the image. - The chart shown focuses on letter recognition and size differentiation, not color perception. *Farnsworth-Munsell hue test* - The **Farnsworth-Munsell hue test** is used for precise **color discrimination** and involves arranging caps of varying hues in a continuum. - This test is distinct from the letter-based visual acuity chart shown in the image. *Pelli-Robson chart* - The **Pelli-Robson chart** is used to measure **contrast sensitivity**, presenting letters of a constant size but decreasing contrast. - While it uses letters, the chart in the image has letters of decreasing size, indicating a visual acuity test rather than contrast sensitivity.
Question 5: Identify the stain instilled in the eye in the following image:
- A. Fluorescein stain (Correct Answer)
- B. Rose Bengal stain
- C. Lissamine green stain
- D. Rhodamine stain
Explanation: ***Fluorescein stain*** - The image shows a **green-yellow fluorescence** under cobalt blue light, which is characteristic of **fluorescein dye** pooling in areas of epithelial defect or healthy tear film. - Fluorescein is a commonly used diagnostic dye in ophthalmology to visualize **corneal abrasions**, ulcers, or contact lens-related issues as it stains damaged corneal epithelial cells. *Rose Bengal stain* - **Rose Bengal** stains devitalized epithelial cells and mucus a **red or purple color**, not green or yellow. - It is particularly useful for identifying **dry eye syndrome** and herpes simplex keratitis but would appear distinctly different from the image. *Lissamine green stain* - **Lissamine green** stains damaged or devitalized conjunctival and corneal cells a **blue-green color**, similar to Rose Bengal. - While it has a greenish hue, it typically does not fluoresce and produces a distinct staining pattern different from the bright, uniform green seen with fluorescein under blue light. *Rhodamine stain* - **Rhodamine** dyes, which are typically **red or pink fluorescent**, are not routinely used as a standard ophthalmic stain for general corneal evaluation. - Its spectral properties and clinical applications are distinct from the common diagnostic dyes used on the ocular surface.
Question 6: A patient from slum presents with grittiness in eyes. Everted eyelid shows: (Recent NEET Pattern 2016-17)
- A. Trachoma (Correct Answer)
- B. Vernal conjunctivitis
- C. Eales disease
- D. Phlyctenular keratoconjunctivitis
Explanation: ***Trachoma*** - The image shows **conjunctival follicles** and **gritty sensation** in a patient from a slum, which are classic signs of Trachoma caused by *Chlamydia trachomatis*. The everted eyelid typically reveals these characteristic follicles. - Trachoma is prevalent in areas with **poor sanitation** and **limited access to water**, consistent with a "slum" setting. *Vernal conjunctivitis* - Characterized by **giant papillae (cobblestone papillae)** on the upper tarsal conjunctiva, often associated with a history of allergies and intense itching. - While it can cause grittiness, the picture does not show the typical giant papillae, but rather smaller, more numerous follicles. *Eales disease* - This is an **idiopathic inflammatory vaso-occlusive disease** affecting the retinal vessels, primarily in young adult males. - It presents with **recurrent vitreous hemorrhages and retinal detachment**, not primarily with conjunctival findings or grittiness. *Phlyctenular keratoconjunctivitis* - Involves the formation of **phlyctenules** (small, nodular lesions) on the conjunctiva or cornea, often associated with delayed hypersensitivity to microbial antigens, such as *Staphylococcus* or *Mycobacterium tuberculosis*. - While it can cause grittiness and photophobia, the follicular pattern in the image is not typical of phlyctenules.
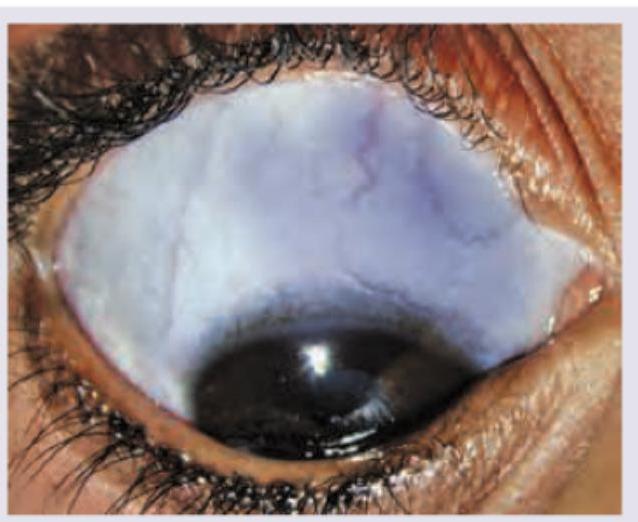
Question 7: All are causes of the presentation shown below except:
- A. Marfan syndrome
- B. Ehlers-Danlos syndrome
- C. Buphthalmos (Correct Answer)
- D. High hypermetropia
Explanation: ***Buphthalmos*** - **Buphthalmos** refers to congenital glaucoma causing **enlargement of the eyeball** with increased corneal diameter (>12 mm). - Classical features include **corneal edema**, **Haab's striae**, and **increased intraocular pressure**. - Buphthalmos does **NOT cause blue sclera**. The sclera in congenital glaucoma is typically normal in color, though the enlarged globe and corneal changes are prominent. - This is the correct answer as it does not cause the presentation shown (blue sclera). *Marfan syndrome* - **Marfan syndrome** is a genetic disorder affecting **fibrillin-1**, leading to connective tissue abnormalities. - Causes **scleral thinning** resulting in **blue sclera** due to visualization of underlying choroidal pigment. - Other ocular features include **ectopia lentis** (upward lens subluxation), **myopia**, and **retinal detachment**. - Systemic features: aortic root dilation, tall stature, arachnodactyly, pectus deformities. *Ehlers-Danlos syndrome* - A group of inherited connective tissue disorders with **collagen defects** (various types affecting different collagen types). - Causes **blue sclera** due to **scleral thinning** and transparency. - Other features include **skin hyperextensibility**, **joint hypermobility**, **tissue fragility**, and easy bruising. - Ocular complications: keratoconus, retinal detachment, globe rupture with minimal trauma. *High hypermetropia* - While **high hypermetropia** primarily refers to a refractive error with light focusing behind the retina, in the context of this question it likely refers to conditions with **nanophthalmos** (abnormally small eye). - Some forms of **microphthalmos with nanophthalmos** can have associated **scleral thickening or abnormalities** that may give a bluish appearance in rare syndromic cases. - However, this association is tenuous compared to the clear connective tissue disorders listed above.
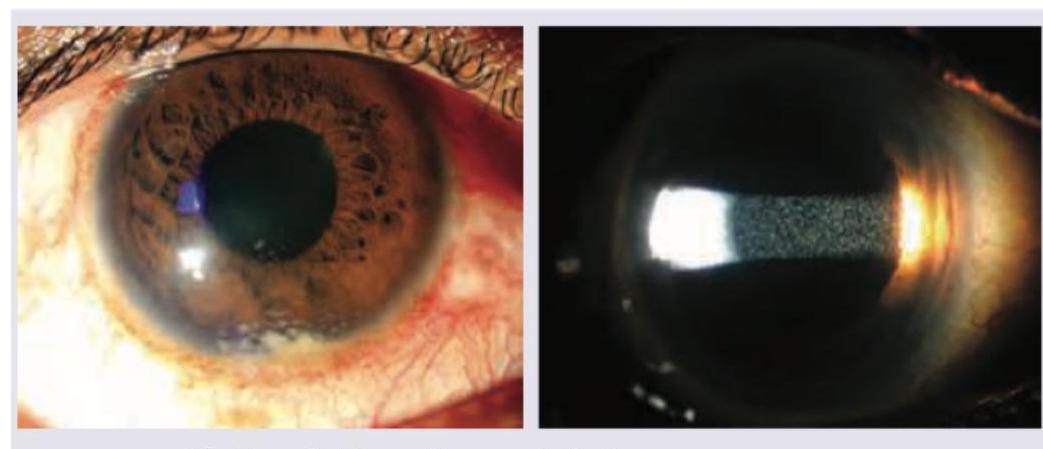
Question 8: A 30-year-old school teacher presents with complaints of red eye with photophobia. Ocular findings are shown below. All are true about the condition shown except: (Recent NEET Pattern 2016-17)
- A. Mutton-fat keratic precipitates
- B. Dalen-Fuchs nodules
- C. Aqueous flare
- D. Muddy iris (Correct Answer)
Explanation: ***Muddy iris*** - A "muddy iris" appearance refers to loss of the normal iris architecture and fine details due to **diffuse iris stromal edema** - This is a characteristic feature of **non-granulomatous (acute) anterior uveitis**, not granulomatous uveitis - The images show **granulomatous anterior uveitis** (evidenced by mutton-fat KPs), where muddy iris is typically **absent** or less prominent - **This is the correct answer** as it is NOT a typical feature of the condition shown *Mutton-fat keratic precipitates* - The left image shows large, greasy-looking deposits on the corneal endothelium - These are characteristic **mutton-fat keratic precipitates (KPs)** composed of macrophages and epithelioid cells - These are **pathognomonic for granulomatous uveitis** and are clearly visible in the condition shown *Dalen-Fuchs nodules* - These are yellowish-white collections of lymphocytes and epithelioid cells between **Bruch's membrane and the RPE** in the peripheral fundus - They are a feature of **granulomatous posterior uveitis**, particularly in **Vogt-Koyanagi-Harada (VKH) disease** and sympathetic ophthalmia - While not visible in these anterior segment images, they **can coexist** in patients with granulomatous panuveitis *Aqueous flare* - The right image (slit lamp beam) shows visible **aqueous flare** - cloudiness in the anterior chamber - This indicates **protein leakage** from breakdown of the blood-aqueous barrier - This is a **direct sign of active inflammation** and is commonly seen in both granulomatous and non-granulomatous uveitis
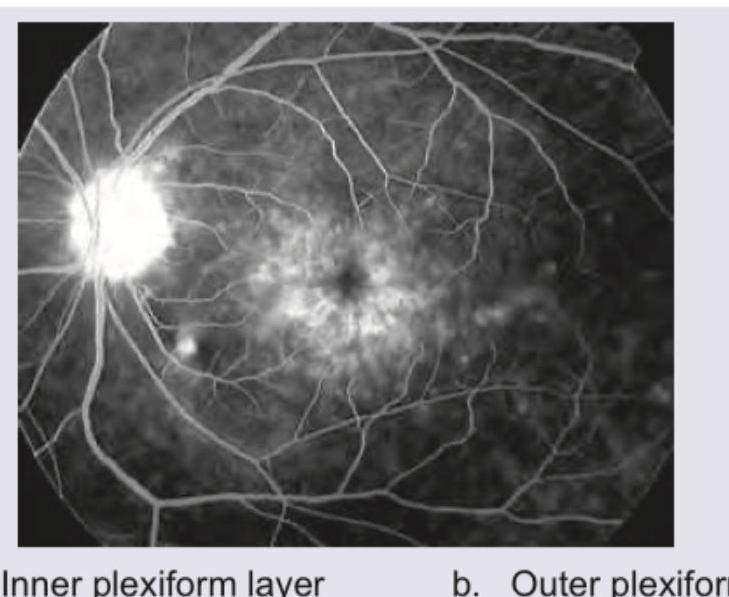
Question 9: The given FFA appearance occurs due to accumulation of dye in which of the following layers of retina?
- A. Inner plexiform layer (Correct Answer)
- B. Outer plexiform layer
- C. Ganglion cell layer
- D. Outer nuclear layer
Explanation: ***Inner plexiform layer*** - In **cystoid macular edema (CME)**, fluid accumulation occurs in multiple retinal layers, with the **inner plexiform layer** and **inner nuclear layer** being significantly involved. - The characteristic **petaloid (flower-petal) pattern** on fluorescein angiography results from fluid accumulation arranged around the foveal center in a radial pattern. - The **Müller cells**, which span the retina vertically, contribute to the formation of cystoid spaces when their supporting function is disrupted. **Note:** While the **outer plexiform layer (Henle's layer)** is classically described as the primary site of CME in many textbooks due to the radial arrangement of Henle fibers, fluid accumulation also prominently involves the **inner nuclear and inner plexiform layers**, and different imaging modalities and stages of CME may show variable involvement. *Outer plexiform layer* - The outer plexiform layer (also called **Henle's layer** at the macula) is frequently cited as a primary site of fluid accumulation in CME. - The radial arrangement of photoreceptor axons (Henle fibers) in this layer can contribute to the characteristic petaloid pattern. - Modern OCT imaging often shows cystoid spaces involving both outer plexiform and inner nuclear layers. *Ganglion cell layer* - The ganglion cell layer is the most superficial retinal layer containing neuronal cell bodies. - This layer is **not typically involved** in the cystoid fluid accumulation pattern of CME. - Edema here would present differently, potentially obscuring vessels or causing diffuse thickening. *Outer nuclear layer* - The outer nuclear layer contains photoreceptor cell bodies (nuclei of rods and cones). - This layer is **not characteristically involved** in CME's petaloid pattern. - Fluid in this layer is more associated with conditions like **outer retinal edema**, **retinoschisis**, or certain forms of retinal detachment.
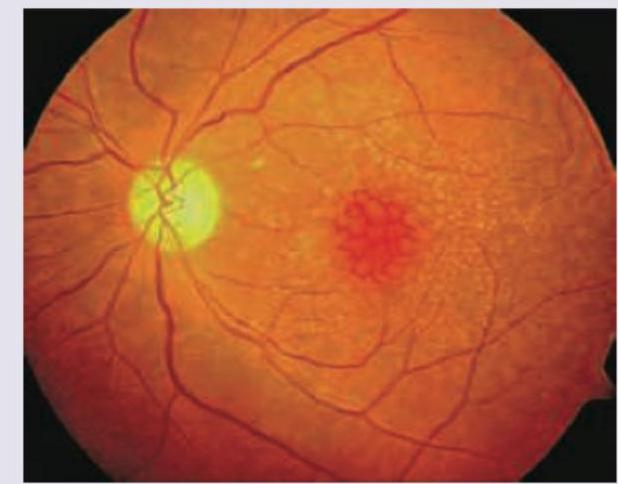
Question 10: A 75-year-old Englishman living in India presents to OPD with complaints of gradual onset painless, progressive blurring of central vision. He says he could earlier drive to the hospital by himself but is not able to do so now. Slit lamp examination is normal. Fundus examination is given below. What is the diagnosis?
- A. Central serous retinopathy
- B. Cystoid macular edema
- C. Rhegmatogenous retinal detachment
- D. Age-related macular degeneration (Correct Answer)
Explanation: ***Age-related macular degeneration*** - The patient's age (75 years), gradual painless progressive blurring of **central vision**, and the presence of **drusen** (small yellow deposits) and a **macular hemorrhage** (red spot) on the fundus exam are all characteristic features of wet age-related macular degeneration. - The inability to drive due to vision loss further points to significant central vision impairment, which is a hallmark of AMD, especially the wet form due to **neovascularization** and hemorrhage. *Central serous retinopathy* - Typically affects younger to middle-aged individuals, often associated with stress or corticosteroid use, contrasting with the patient's age. - Characterized by **serous fluid detachment** of the neurosensory retina, not usually significant hemorrhage as seen in the image. *Cystoid macular edema* - Presents with **cyst-like fluid accumulation** within the retina, often leading to a flower petal-like appearance on imaging, which is not depicted in this fundus image. - Can be associated with various conditions like diabetes, retinal vein occlusion, or inflammation, and while it causes central vision loss, the funduscopic appearance here is more consistent with AMD. *Rhegmatogenous retinal detachment* - Usually presents with sudden vision loss, **floaters**, or **flashes of light**, and a "curtain" coming over the vision, which differs from the gradual onset described. - Fundus examination would typically show a detached, billowing retina, often with a retinal tear, not the macular changes with drusen and hemorrhage seen here.