NEET-PG 2017 — Obstetrics and Gynecology
20 Previous Year Questions with Answers & Explanations
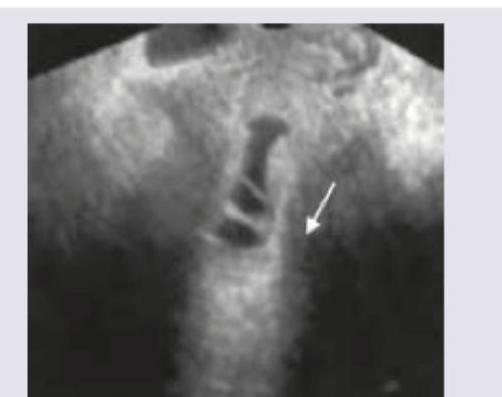
A pregnant woman undergoes a routine antenatal ultrasound scan in the second trimester. The sonologist notes an abnormal appearance of the fetal skull. What is the sign demonstrated in the given antenatal USG image?

Transvaginal saline infusion sonographic evaluation shows:

What is the best treatment for the condition shown below?
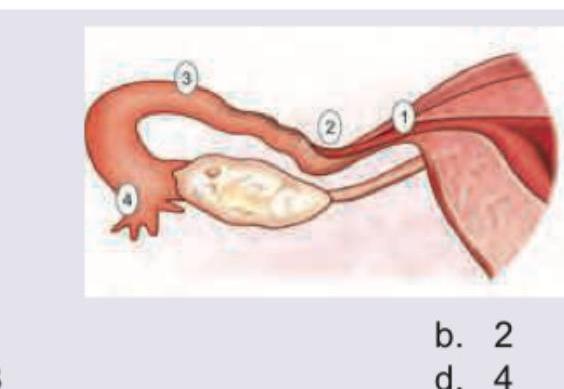
A 25-year-old lady had tubal rupture due to ectopic pregnancy at 6 weeks. The most common site of rupture of ectopic pregnancy amongst the following is:
The image shows:
Which is incorrect about the presentation shown below?
Which is the least common type of pelvis out of the types shown below?
Which of the following is correct about the placenta shown below? (Recent NEET Pattern 2016-17)
What is the type of placenta previa shown below?
The image shows:
NEET-PG 2017 - Obstetrics and Gynecology NEET-PG Practice Questions and MCQs
Question 1: A pregnant woman undergoes a routine antenatal ultrasound scan in the second trimester. The sonologist notes an abnormal appearance of the fetal skull. What is the sign demonstrated in the given antenatal USG image?
- A. Boomerang sign
- B. Spring coiled sign
- C. Banana sign
- D. Lemon sign (Correct Answer)
Explanation: ***Lemon sign*** - The **lemon sign** refers to the shape of the fetal skull on ultrasound, where the frontal bones are indented, making the head appear lemon-shaped. - This sign is often associated with **Chiari II malformation** and spina bifida, where there is downward displacement of the cerebellar vermis and fourth ventricle. *Boomerang sign* - The **boomerang sign** is typically observed in imaging of the knee, referring to a meniscal tear where the displaced fragment resembles a boomerang. - It is not a sign used for fetal cranial abnormalities in ultrasound. *Spring coiled sign* - The **spring coiled sign** is a feature seen in intussusception on ultrasound, where layers of bowel are invaginated within another, resembling a coiled spring. - This sign is related to intestinal pathology, not fetal head anomalies. *Banana sign* - The **banana sign** describes the appearance of the cerebellum on fetal ultrasound when it is displaced or compressed due to Chiari II malformation, making it appear banana-shaped. - While also associated with Chiari II, the image provided shows the **head shape**, not the cerebellum, aligning with the lemon sign.
Question 2: Transvaginal saline infusion sonographic evaluation shows:
- A. Submucous leiomyoma
- B. Cervical stenosis
- C. PCOD
- D. Asherman's syndrome (Correct Answer)
Explanation: ***Asherman's syndrome*** - The image shows **intracavitary adhesions** within the endometrial cavity, characterized by bridging bands or strands of tissue with an irregular endometrial surface, as indicated by the arrow. - These findings on **saline infusion sonography (SIS)** are highly suggestive of **Asherman's syndrome**, which involves the formation of intrauterine adhesions. *Submucous leiomyoma* - Submucous leiomyomas (submucosal fibroids) are fibroids that project into the endometrial cavity and typically appear as **well-defined, hypoechoic masses** that distort the cavity. - The image does not show a distinct mass but rather **irregular strands** and a distorted cavity indicative of adhesions, not a fibroid. *Cervical stenosis* - Cervical stenosis involves an **abnormal narrowing of the cervical canal**, which would be seen as an obstruction to fluid flow into the uterine cavity during SIS. - While the image shows fluid within the uterine cavity, the primary pathology is within the cavity itself, not merely an obstruction at the cervix. *PCOD* - **Polycystic ovary syndrome (PCOS)** is primarily an ovarian disorder characterized by **multiple small follicles** (cysts) in the ovaries and hormonal imbalances. - PCOS is not a condition diagnosed by evaluating the endometrial cavity for adhesions using saline infusion sonography.
Question 3: What is the best treatment for the condition shown below?
- A. Hysteroscopic adhesiolysis (Correct Answer)
- B. OCP
- C. Transvaginal hysterectomy
- D. Intrauterine hyaluronidase injection
Explanation: ***Hysteroscopic adhesiolysis*** - The image shows an **intrauterine synechia**, also known as an **Asherman syndrome** or uterine adhesion, which manifests as fibrous bands within the uterine cavity (indicated by the arrow). - **Hysteroscopic adhesiolysis** is the gold standard for treating intrauterine adhesions, involving the surgical removal of these adhesions under direct visualization to restore the uterine cavity's normal anatomy. *OCP* - **Oral contraceptive pills (OCPs)** are primarily used for contraception, managing menstrual irregularities, or hormonal therapy. - They do not address or resolve **intrauterine adhesions** causing conditions like Asherman syndrome. *Transvaginal hysterectomy* - A **transvaginal hysterectomy** involves the surgical removal of the entire uterus, which is an aggressive and irreversible procedure. - This is not an appropriate treatment for intrauterine adhesions, especially in patients who may desire future fertility. *Intrauterine hyaluronidase injection* - While hyaluronidase is an enzyme that breaks down hyaluronic acid and has been explored in various applications, its efficacy as a primary treatment for established **intrauterine adhesions** is not well-supported in clinical practice. - The **mechanical removal** of fibrous adhesions is typically required.
Question 4: A 25-year-old lady had tubal rupture due to ectopic pregnancy at 6 weeks. The most common site of rupture of ectopic pregnancy amongst the following is:
- A. 1
- B. 2 (Correct Answer)
- C. 3
- D. 4
Explanation: ***Option 2 (Ampulla)*** - The image shows the **ampulla** of the fallopian tube labeled with '2'. This is the **most common site** for ectopic pregnancies, accounting for approximately **80-90%** of all tubal ectopic pregnancies. - The ampulla is the widest and longest part of the fallopian tube, making it a frequent location for implantation outside the uterus. Despite being wider, rupture is common here due to the thin wall and progressive distension from the growing pregnancy. *Option 1 (Interstitial/Cornual)* - The image points to the **interstitial** (or cornual) portion of the fallopian tube, labeled '1'. This is the **least common site** for ectopic pregnancy, accounting for only **2-4%** of cases. - While rare, rupture here can be **catastrophic** due to proximity to the uterine blood supply and rich vascular anastomoses, leading to severe hemorrhage. *Option 3 (Isthmus)* - The image highlights the **isthmus** of the fallopian tube with '3'. Ectopic pregnancies in the isthmus account for approximately **12%** of cases. - Rupture in the isthmus typically occurs **earlier** (around 6-8 weeks) than in the ampulla due to its narrower lumen and thicker muscular wall, which limits its ability to accommodate the growing pregnancy. *Option 4 (Infundibulum/Fimbriae)* - The image points to the **infundibulum** and **fimbriae**, labeled '4'. Fimbrial ectopic pregnancies are **extremely rare**, accounting for less than **5%** of cases. - The fimbriae are involved in capturing the ovum after ovulation. Implantation here is uncommon and may result in fimbrial abortion rather than rupture.
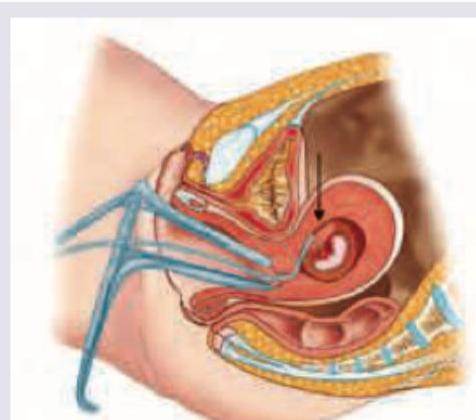
Question 5: The image shows:
- A. PUBS (Correct Answer)
- B. Amniocentesis
- C. Chorionic villus sampling
- D. Fetal scalp sampling
Explanation: **PUBS** - The image displays a procedure where a needle is inserted through the maternal abdomen and into the **umbilical cord blood vessel** of the fetus, which is characteristic of **Percutaneous Umbilical Blood Sampling (PUBS)**. - PUBS, also known as **cordocentesis**, is used to obtain fetal blood for diagnostic purposes, such as detecting chromosomal abnormalities, genetic disorders, or fetal infections. *Amniocentesis* - **Amniocentesis** involves sampling **amniotic fluid** from the sac surrounding the fetus, not directly from the umbilical cord. - The needle in amniocentesis typically targets the amniotic sac, while in the image, it clearly targets an umbilical vessel. *Chorionic villus sampling* - **Chorionic villus sampling (CVS)** involves obtaining tissue from the **placenta** (chorionic villi), either transabdominally or transcervically. - The image clearly shows the needle entering the umbilical cord, not the placental tissue. *Fetal scalp sampling* - **Fetal scalp sampling** is performed during labor to assess fetal well-being by analyzing **fetal blood pH** from a small incision on the fetal scalp. - This procedure is performed late in pregnancy during labor and involves accessing the fetal scalp via the cervix, which is distinct from the transabdominal umbilical cord access shown.
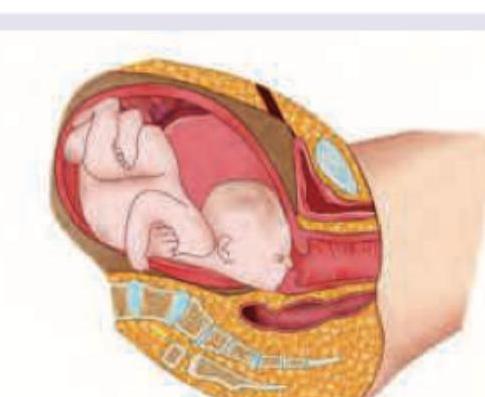
Question 6: Which is incorrect about the presentation shown below?
- A. Associated with anencephaly
- B. Mark commonly seen with platypelloid pelvis (Correct Answer)
- C. Head is partially extended
- D. Vaginal delivery is possible
Explanation: ***Mark commonly seen with platypelloid pelvis*** - The image shows a **brow presentation**, where the fetal head is incompletely extended, with the **forehead (bregma to root of nose)** presenting. - A **platypelloid pelvis** (flat pelvis) is characterized by a wide transverse diameter and a short anteroposterior diameter, which typically **favors transverse lie or occipito-transverse positions**, NOT brow presentation. - Brow presentation is more commonly associated with **cephalopelvic disproportion, anencephaly, multiparity, prematurity**, and other factors that prevent proper head flexion. *Associated with anencephaly* - This statement is **correct**. Brow presentation is indeed more common in fetuses with **anencephaly** due to the absence of the cranial vault, which alters fetal head mechanics and prevents normal flexion. - The altered head shape and lack of cranial vault prevent proper flexion, leading to the forehead becoming the presenting part. *Head is partially extended* - This statement is **correct**. In a **brow presentation**, the fetal head is in a state of **partial or incomplete extension**, positioned between full flexion (vertex) and full extension (face presentation). - The presenting diameter is the **mento-vertical diameter** (approximately 13-13.5 cm), which is the largest diameter and often leads to cephalopelvic disproportion. - If the head were fully extended, it would be a **face presentation** (mentum presenting); if fully flexed, it would be a **vertex presentation** (occiput presenting). *Vaginal delivery is possible* - This statement is **correct**. While **brow presentations** often lead to **cephalopelvic disproportion** and commonly require Cesarean section, vaginal delivery is possible in certain circumstances: - If the head **flexes** to a vertex presentation during labor - If the head **extends** to a face presentation during labor - If the fetus is small and the pelvis is adequately capacious - However, **persistent brow presentations** are associated with significantly increased risk of obstructed labor, maternal trauma, and perinatal morbidity, usually necessitating operative delivery.
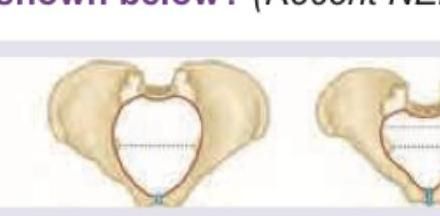
Question 7: Which is the least common type of pelvis out of the types shown below?
- A. 1
- B. 3 (Correct Answer)
- C. 2
- D. 4
Explanation: ***3*** - Pelvis type 3, the **platypelloid** pelvis, is characterized by a **flattened oval inlet**, with a short anteroposterior diameter and a wide transverse diameter. - It is the **least common** type in women, representing only about **3-5%** of female pelves, and is associated with difficulties in engagement and descent of the fetal head due to the reduced anteroposterior diameter. *1* - Pelvis type 1, the **gynecoid** pelvis, is the most common and **ideal for childbirth**, found in about 50% of women. - It features a **round or slightly oval inlet**, and a wide sacrosciatic notch and subpubic angle, making it well-suited for vaginal delivery. *2* - Pelvis type 2, the **anthropoid** pelvis, has an **oval inlet** that is longer in the anteroposterior diameter than the transverse. - This type occurs in about 20-30% of women and can allow for successful vaginal delivery, often with the fetus in an occipitoposterior position. *4* - Pelvis type 4, the **android** pelvis, is characterized by a **heart-shaped inlet** and a narrow subpubic angle. - It occurs in about 20-30% of female pelves and is associated with more difficult labor due to the narrow mid-pelvis and convergent side walls.
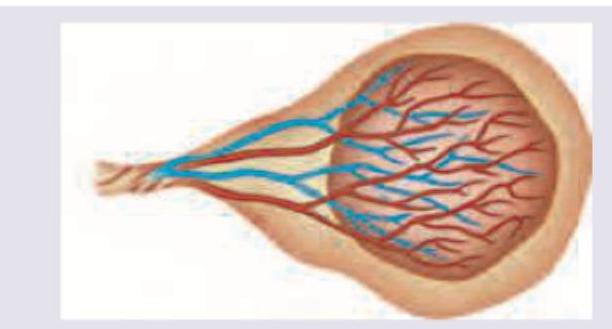
Question 8: Which of the following is correct about the placenta shown below? (Recent NEET Pattern 2016-17)
- A. Velamentous cord insertion
- B. Battledore placenta (Correct Answer)
- C. Placental chorioangioma
- D. Circumvallate placenta
Explanation: ***Battledore placenta*** - This image depicts a **marginal insertion of the umbilical cord** into the placenta, where the cord attaches to the edge rather than the center or a more central part of the placental disc. This is characteristic of a battledore placenta. - The name "battledore" refers to the resemblance of the placenta and cord to a **tennis racket (battledore)**, where the cord is the handle and the placenta is the head. *Velamentous cord insertion* - In velamentous insertion, the **umbilical vessels diverge in the membranes before reaching the placental disc**, making them unprotected. - In this image, the cord clearly inserts into the edge of the placenta, rather than having vessels spread out in the membranes. *Placental chorioangioma* - A placental chorioangioma is a **benign tumor of the placenta**, characterized by an abnormal proliferation of fetal vessels within the chorionic villi. - This condition is a **mass within the placenta** itself and is not depicted by an anomalous cord insertion pattern. *Circumvallate placenta* - A circumvallate placenta has a **thickened, rolled amnion and chorion** due to a fold of the fetal membranes on the fetal side limiting the expansion of the placenta. - This describes a **membrane abnormality** affecting the shape of the placenta, not directly related to the cord insertion site shown.
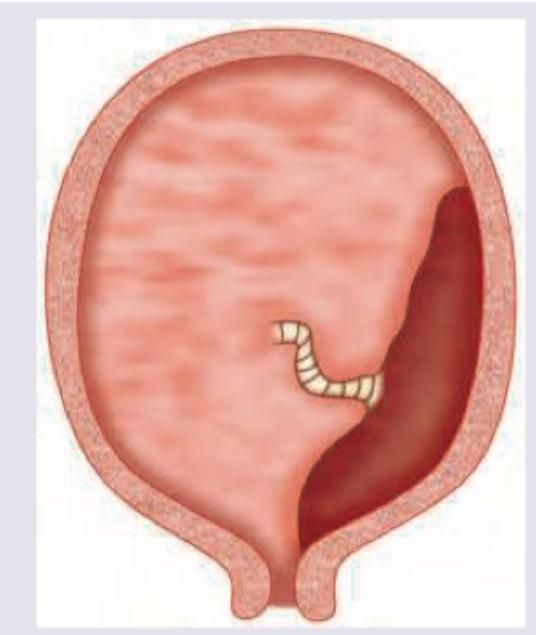
Question 9: What is the type of placenta previa shown below?
- A. Type 1
- B. Type 2
- C. Type 3
- D. Type 4 (Correct Answer)
Explanation: ***Type 4*** - Type 4 placenta previa, also known as **complete or central placenta previa**, occurs when the **placenta completely covers the internal cervical os**. - This type necessitates a **cesarean section** delivery due to the complete obstruction of the birth canal. *Type 1* - Type 1 placenta previa, or **low-lying placenta**, means the placenta is in the lower uterine segment but **does not reach the cervical os**. - It often resolves by term as the uterus grows, potentially allowing a **vaginal delivery**. *Type 2* - Type 2 placenta previa, or **marginal placenta previa**, indicates the placental edge **reaches the internal cervical os** but does not cover it. - While a vaginal delivery might be possible, there's an increased risk of **hemorrhage**. *Type 3* - Type 3 placenta previa, or **partial placenta previa**, is where the placenta **partially covers the internal cervical os** but not completely. - This type also typically requires a **cesarean section** due to the obstruction.
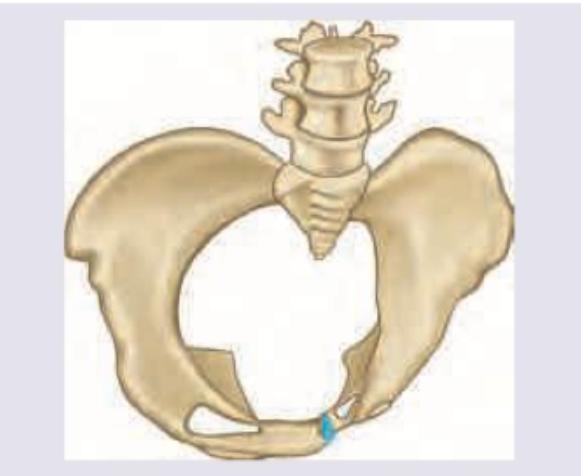
Question 10: The image shows:
- A. Scoliotic pelvis
- B. Osteomalacic pelvis
- C. Naegele pelvis
- D. Rachitic pelvis (Correct Answer)
Explanation: ***Rachitic pelvis*** - The image illustrates a **flattened anteroposterior diameter** and a **pronounced protrusion of the sacrum** into the pelvic cavity. - These features are characteristic of a rachitic pelvis, which results from **rickets** (vitamin D deficiency) in childhood, leading to softened bones and deformities due to gravitational and muscular forces. *Scoliotic pelvis* - A scoliotic pelvis would show **asymmetry** in the pelvic bones due to **lateral curvature of the spine**, which is not the primary symmetrical flattening seen here. - This condition involves a **twisting or rotation** of the pelvis, rather than the anteroposterior compression depicted. *Osteomalacic pelvis* - An osteomalacic pelvis, while also due to poor bone mineralization, typically presents with a **triradiate or trefoil shape** resulting from indentation of the acetabula and collapse of the sacrum into the pelvic canal, leading to a **heart-shaped inlet**. - While related to vitamin D deficiency, the specific deformation pattern in the image with characteristic flattening is more indicative of a rachitic pelvis from childhood rather than adult-onset osteomalacia. *Naegele pelvis* - A Naegele pelvis is an **obliquely contracted pelvis** characterized by **atrophy or absence of one sacral ala** and ankylosis of the corresponding sacroiliac joint. - This results in a highly asymmetrical, severely distorted pelvic inlet, which is distinct from the symmetrical flattening observed in the image.