NEET-PG 2017 — Internal Medicine
13 Previous Year Questions with Answers & Explanations
A 68-year-old postoperative patient who has undergone thyroidectomy presents with muscle cramps. ECG shows?
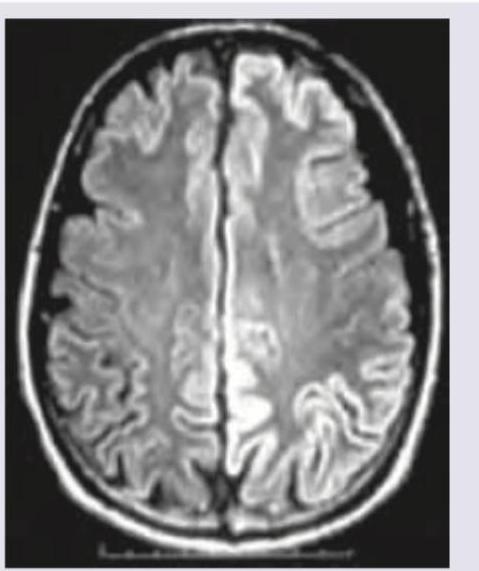
MRI was performed on a 35-year-old man with progressive myoclonus and apathy. What is the diagnosis? (Recent NEET Pattern 2016-17)
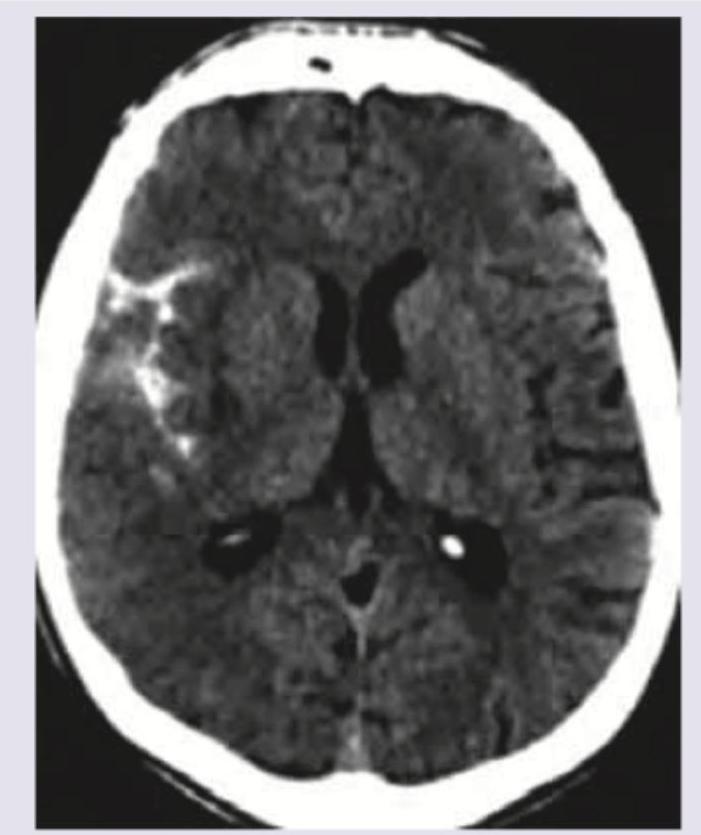
A 35-year-old woman presents with thunderclap headache. NCCT was done. All are true about the condition except:
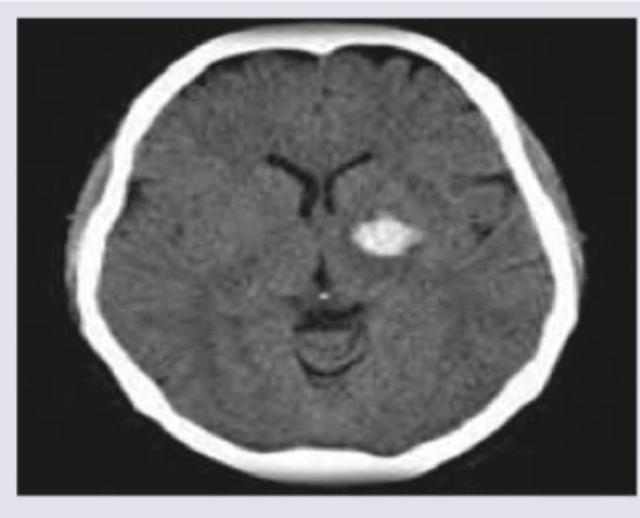
A 50-year-old hypertensive patient develops sudden onset drooping of right face and hemiplegia. What is the diagnosis?
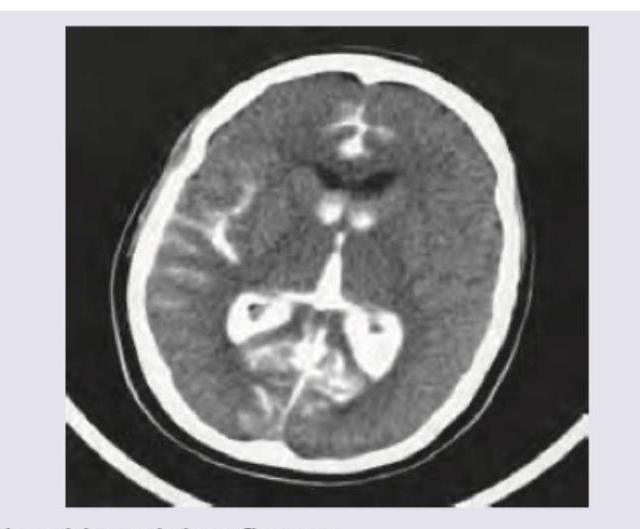
A patient presents with GCS of 7 with nuchal rigidity and bloody CSF. Which is incorrect regarding this condition? (Recent NEET Pattern 2016-17)
A patient of swine flu has developed severe respiratory distress. Which of the following findings confirm the diagnosis of ARDS in this patient?
A 40-year-old woman with history of progressive shortness of breath has lesions on her legs as shown. HbA1C of the patient is 5.8%. Lipid profile shows serum cholesterol 175 mg%. What is the diagnosis? (Recent NEET Pattem 2016-17)

The EEG of the patient shows which of the following? (Recent NEET Pattern 2016-17)
The EEG of a 16-year-old boy with early morning involuntary movements of hands in his sleep noticed by parents, was performed. Immunization is complete. What does EEG show? (Recent NEET Pattern 2016-17)
Which of the following infections in most commonly seen in this transfusion dependant child shown below?
NEET-PG 2017 - Internal Medicine NEET-PG Practice Questions and MCQs
Question 1: A 68-year-old postoperative patient who has undergone thyroidectomy presents with muscle cramps. ECG shows?
- A. Prolonged QT interval (Correct Answer)
- B. Short QT interval
- C. ST elevation
- D. ST depression
Explanation: ***Prolonged QT interval*** - A patient who has undergone thyroidectomy and presents with muscle cramps likely has **hypocalcemia** due to inadvertent parathyroid gland removal. - Hypocalcemia is well-known to cause a **prolonged QT interval** on EKG, increasing the risk of arrhythmias. *Short QT interval* - A short QT interval is typically associated with **hypercalcemia** or genetic disorders. - This patient's presentation of muscle cramps is inconsistent with hypercalcemia. *ST elevation* - ST elevation is a hallmark of **acute myocardial infarction** or **pericarditis**. - This finding is unrelated to hypocalcemia or the patient's immediate postoperative and symptoms. *ST depression* - ST depression often indicates **myocardial ischemia** or **digoxin effect**. - It is not a characteristic ECG change associated with hypocalcemia or muscle cramps.
Question 2: MRI was performed on a 35-year-old man with progressive myoclonus and apathy. What is the diagnosis? (Recent NEET Pattern 2016-17)
- A. Herpes simplex encephalitis
- B. SSPE
- C. Mesial temporal sclerosis
- D. Prion disease (Correct Answer)
Explanation: ***Prion disease*** - The MRI shows **cortical ribboning** (hyperintensity in the cortex) and possible signal changes in the basal ganglia, which are characteristic findings in prion diseases such as **Creutzfeldt-Jakob disease (CJD)**. - The clinical presentation of **progressive myoclonus** (sudden, involuntary muscle jerks) and **apathy** (lack of emotion or motivation), especially in a relatively young individual (35 years old), is highly suggestive of CJD or another prion disease. *Herpes simplex encephalitis* - This typically presents with **fever, headache, and focal neurological deficits**, often affecting the **temporal lobes**. - While it can cause FLAIR hyperintensities, it usually begins acutely with more prominent edema and may have hemorrhagic components, and myoclonus is not a primary defining symptom. *SSPE* - **Subacute sclerosing panencephalitis (SSPE)** is a rare, fatal, progressive brain disorder caused by the **measles virus**, primarily affecting children and young adults. - While it can cause progressive neurological deterioration and cognitive decline, myoclonus is often a late feature, and MRI findings often show **white matter demyelination** in later stages, which is not the predominant finding here. *Mesial temporal sclerosis* - This condition is characterized by **atrophy and signal changes in the hippocampus and amygdala** on MRI, typically associated with **temporal lobe epilepsy**. - While it can cause cognitive issues, it usually does not account for widespread cortical ribboning or prominent myoclonus in this age group, and the image does not specifically highlight mesial temporal lobe changes.
Question 3: A 35-year-old woman presents with thunderclap headache. NCCT was done. All are true about the condition except:
- A. Hyponatremia
- B. Prolonged QT interval
- C. Most common cause of death is rebleeding (Correct Answer)
- D. Nimodipine is drug of choice
Explanation: The image provided appears to be a **Non-Contrast CT (NCCT) scan of the brain**, showing a **hyperdense area** in the right hemisphere, consistent with **subarachnoid hemorrhage (SAH)** given the context of a "thunderclap headache." Thunderclap headache is a classic symptom of SAH. ***Most common cause of death is rebleeding*** - While rebleeding is a **serious complication** and contributes significantly to morbidity and mortality in SAH patients, the most common cause of death following SAH, particularly in the acute phase, is often related to the **initial hemorrhage** itself, such as **brain herniation**, or **early hydrocephalus** and **vasospasm-induced cerebral ischemia**. - **Vasospasm**, leading to **delayed cerebral ischemia (DCI)**, is a major cause of death and disability in SAH survivors, but the question asks about the "most common cause of death," which in many cases is the immediate devastating effect of the initial bleed or its early complications rather than rebleeding alone. *Hyponatremia* - **Hyponatremia** is a common electrolyte imbalance seen in patients with SAH, often due to **Syndrome of Inappropriate Antidiuretic Hormone (SIADH)** or **Cerebral Salt Wasting (CSW)**. - Therefore, the statement that hyponatremia occurs is **true** for this condition. *Prolonged QT interval* - **Cardiac abnormalities**, including **ECG changes** such as **QT prolongation**, T-wave inversion, and ST depression, are frequently observed after SAH due to **autonomic nervous system dysfunction** and catecholamine release. - Therefore, the presence of a prolonged QT interval is **true** for this condition. *Nimodipine is drug of choice* - **Nimodipine** is a **calcium channel blocker** widely used in SAH patients to **prevent or reduce the severity of cerebral vasospasm** and associated delayed cerebral ischemia. - It is currently the **drug of choice** for this indication in SAH, making this statement **true**.
Question 4: A 50-year-old hypertensive patient develops sudden onset drooping of right face and hemiplegia. What is the diagnosis?
- A. MCA area hemorrhage (Correct Answer)
- B. ACA area infarction
- C. ACA area hemorrhage
- D. MCA area infarction
Explanation: ***MCA area hemorrhage*** - The **hyperdense lesion** on CT scan indicates **acute hemorrhage** in the MCA territory, which correlates with the sudden onset right facial droop and hemiplegia. - **Hypertension** is the most common risk factor for primary **intracerebral hemorrhage**, and MCA territory involvement typically causes contralateral face and arm weakness. *MCA area infarction* - **Infarctions** appear as **hypodense (dark) areas** on CT scan, not hyperdense lesions as described in this case. - While MCA infarction can cause similar clinical symptoms, the imaging findings clearly show hemorrhage rather than ischemic changes. *ACA area infarction* - **ACA infarction** typically presents with **leg weakness** more prominent than face/arm weakness, as the ACA supplies the medial motor cortex for lower limbs. - The imaging shows a **hyperdense hemorrhage**, not the **hypodense appearance** characteristic of infarction. *ACA area hemorrhage* - **ACA territory hemorrhage** would affect the **frontal lobe**, causing symptoms like leg weakness, **abulia** (lack of motivation), and urinary incontinence. - The clinical presentation of **facial droop and hemiplegia** involving face and arm is more characteristic of **MCA involvement** rather than ACA territory.
Question 5: A patient presents with GCS of 7 with nuchal rigidity and bloody CSF. Which is incorrect regarding this condition? (Recent NEET Pattern 2016-17)
- A. Blood in sylvian fissure
- B. Seizures
- C. Intraventricular extension
- D. IV ceftriaxone (Correct Answer)
Explanation: **IV ceftriaxone** - The clinical presentation of **GCS of 7**, **nuchal rigidity**, and **bloody CSF** is highly suggestive of a **subarachnoid hemorrhage (SAH)**, not a bacterial infection like meningitis. - **Ceftriaxone** is an antibiotic commonly used to treat bacterial meningitis, which is not indicated here as the primary issue is hemorrhage, not infection. *Blood in sylvian fissure* - **Blood in the sylvian fissure** is a common finding in **subarachnoid hemorrhage**, as this area contains major cerebral arteries susceptible to aneurysm rupture. - CT scans often show hyperdense (bright) blood within the sulci and cisterns, including the sylvian fissure. *Seizures* - **Seizures** are a relatively common complication of **subarachnoid hemorrhage**, especially in the acute phase due to blood irritating the cerebral cortex. - They can occur in up to 10-20% of SAH patients and are a significant predictor of poorer outcomes. *Intraventricular extension* - **Intraventricular extension** of blood indicates a more severe hemorrhage and is often associated with a worse prognosis in **subarachnoid hemorrhage**. - The presence of blood within the ventricles can lead to **hydrocephalus** and increased intracranial pressure.
Question 6: A patient of swine flu has developed severe respiratory distress. Which of the following findings confirm the diagnosis of ARDS in this patient?
- A. PaO₂/FiO₂ ratio < 200 and PCWP > 18 mm Hg
- B. PaO₂/FiO₂ ratio < 400 and PCWP > 18 mm Hg
- C. PaO₂/FiO₂ ratio < 100 and PCWP < 18 mm Hg
- D. PaO₂/FiO₂ ratio < 300 and PCWP < 18 mm Hg (Correct Answer)
Explanation: PaO₂/FiO₂ ratio < 300 and PCWP < 18 mm Hg - According to the Berlin definition of ARDS, a PaO₂/FiO₂ ratio less than 300 mmHg indicates impaired gas exchange [1]. - A pulmonary capillary wedge pressure (PCWP) less than 18 mmHg rules out cardiogenic pulmonary edema as the primary cause of respiratory distress, which is essential to diagnose ARDS [1]. PaO₂/FiO₂ ratio < 200 and PCWP > 18 mm Hg - A PaO₂/FiO₂ ratio less than 200 mmHg would indicate severe ARDS, but the elevated PCWP > 18 mm Hg suggests that the primary issue is cardiogenic pulmonary edema, not ARDS. - In ARDS, the problem is non-cardiogenic pulmonary edema secondary to capillary leakage in the lungs, thus a low PCWP is a diagnostic criterion [1]. PaO₂/FiO₂ ratio < 400 and PCWP > 18 mm Hg - A PaO₂/FiO₂ ratio less than 400 mmHg is not a specific criterion for ARDS; the cutoff is 300 mmHg. - An elevated PCWP > 18 mm Hg indicates fluid overload due to cardiac dysfunction, which points away from ARDS. PaO₂/FiO₂ ratio < 100 and PCWP < 18 mm Hg - While a PaO₂/FiO₂ ratio less than 100 mmHg indicates profound hypoxemia consistent with severe ARDS, the diagnosis of ARDS is made at a ratio of < 300 mmHg. - This option describes a very severe form of ARDS but the key diagnostic cutoff for ARDS is < 300 mmHg, not specifically less than 100 mmHg for the confirmation of ARDS per the Berlin definition.
Question 7: A 40-year-old woman with history of progressive shortness of breath has lesions on her legs as shown. HbA1C of the patient is 5.8%. Lipid profile shows serum cholesterol 175 mg%. What is the diagnosis? (Recent NEET Pattem 2016-17)
- A. Necrobiosis lipidoica diabeticorum
- B. Xanthoma
- C. Carotenemia
- D. Erythema nodosum (Correct Answer)
Explanation: ***Erythema Nodosum*** - The image shows **tender, red nodules** primarily on the shins, consistent with the characteristic presentation of erythema nodosum. - While exact values for **HbA1c** and **cholesterol** don't directly diagnose this, erythema nodosum is often associated with systemic conditions, and the patient's progressive shortness of breath prompts further investigation into potential underlying causes. *Necrobiosis lipoidica diabeticorum* - This condition presents as **well-demarcated, yellow-brown patches** with a waxy or atrophic center, often with telangiectasias, not the acute tender nodules seen here. - Although it is associated with **diabetes**, the patient's HbA1c (5.8%) is within the prediabetic range, not typically indicative of established diabetes that commonly precedes significant necrobiosis lipoidica. *Xanthoma* - Xanthomas are **yellowish plaques or nodules** caused by lipid deposits in the skin, which can vary in appearance depending on the type (e.g., eruptive, tendinous, planar). - While hyperlipidemia can cause xanthomas, the patient's **normal cholesterol level** (175 mg%) makes this diagnosis less likely, and the lesions in the image are more erythematous and nodular than typical xanthomas. *Carotenemia* - **Carotenemia** is characterized by a harmless **yellow-orange discoloration of the skin**, particularly on the palms and soles, caused by excessive intake of carotene-rich foods. - This condition does not present with discrete, erythematous nodules as depicted in the image.
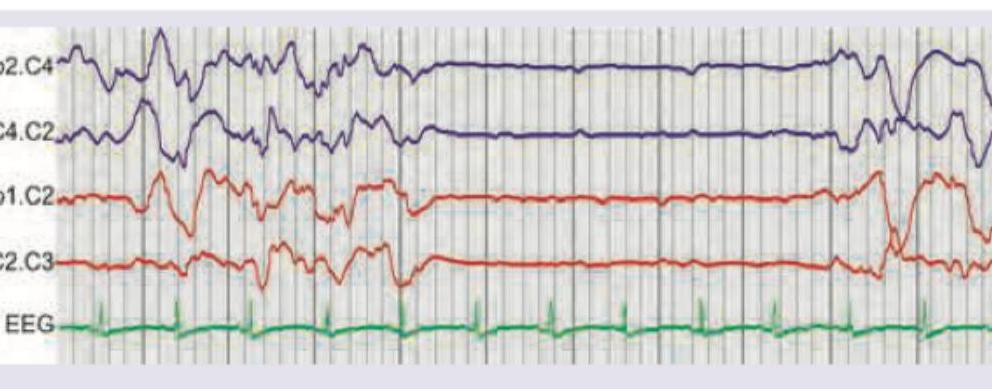
Question 8: The EEG of the patient shows which of the following? (Recent NEET Pattern 2016-17)
- A. Burst suppression pattern (Correct Answer)
- B. Rademecker complex
- C. 3/sec spike and slow wave pattern
- D. 4-6 Hz Polyspike
Explanation: ***Burst suppression pattern*** - The EEG shows periods of high amplitude, mixed-frequency **bursts of activity** alternating with periods of **relative electrical silence** (suppression). - This pattern is often seen in conditions like severe **hypoxic-ischemic encephalopathy**, deep **anesthesia**, or severe brain injury. *Rademecker complex* - This refers to periodic trifasic complexes, often associated with subacute sclerosing panencephalitis (SSPE), which is a **slow viral infection** of the brain. - The complexes are typically **bilateral, synchronous, and repetitive**, not characterized by alternating bursts and suppression. *3/sec spike and slow wave pattern* - This pattern is characteristic of **absence seizures (petit mal epilepsy)**, where there are generalized, synchronous 3 Hz spike-and-wave discharges. - The image does not show continuous, rhythmic 3 Hz activity but rather alternating periods of activity and flat-lining. *4-6 Hz Polyspike* - Polyspikes are a series of two or more spikes or sharp waves clustered together, often associated with **myoclonic seizures** or other generalized epilepsies. - While there are some sharp waves in the burst phases, the overall pattern is dominated by the distinct periods of suppression, not continuous polyspike activity.
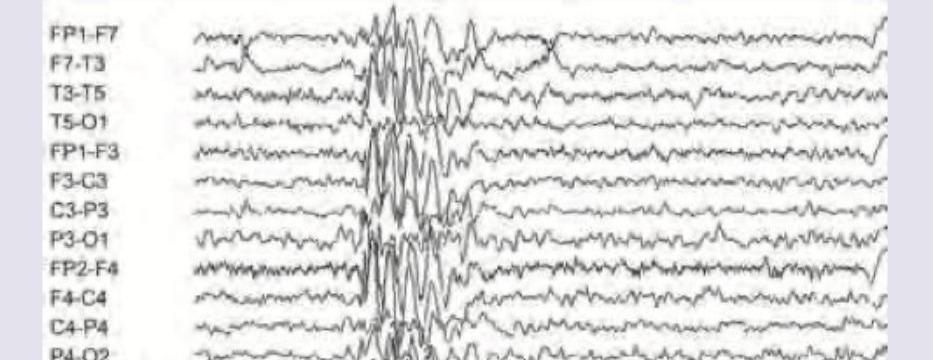
Question 9: The EEG of a 16-year-old boy with early morning involuntary movements of hands in his sleep noticed by parents, was performed. Immunization is complete. What does EEG show? (Recent NEET Pattern 2016-17)
- A. Juvenile myoclonic epilepsy (Correct Answer)
- B. SSPE
- C. Benign rolandic epilepsy
- D. Huntington chorea
Explanation: ***Juvenile myoclonic epilepsy*** - The EEG shows generalized **polyspike-and-slow-wave discharges**, which are characteristic of juvenile myoclonic epilepsy (JME), especially when associated with early morning myoclonus. - The clinical presentation of a **16-year-old boy** with **involuntary movements of hands in his sleep** (suggesting myoclonic jerks), particularly in the morning, is highly consistent with JME. *SSPE* - Subacute sclerosing panencephalitis (SSPE) typically presents with characteristic EEG patterns like **Radermacker complexes** or **periodic complexes**, which are not seen here. - Clinical features of SSPE include progressive cognitive decline, myoclonus, and other neurological deficits, usually following a measles infection, which are not described. *Benign rolandic epilepsy* - Benign rolandic epilepsy (BRE) is characterized by **centrotemporal spikes** on EEG, often exacerbated by sleep, and presents with focal seizures affecting the face and mouth. - The generalized polyspike-and-slow-wave pattern and the clinical description of hand myoclonus do not fit the profile of BRE. *Huntington chorea* - Huntington's chorea is a **neurodegenerative genetic disorder** characterized by involuntary movements (chorea), cognitive decline, and psychiatric problems. - EEG findings in Huntington's chorea are often non-specific or show generalized slowing, and it is not an epilepsy syndrome with specific high-amplitude epileptiform discharges like those seen.
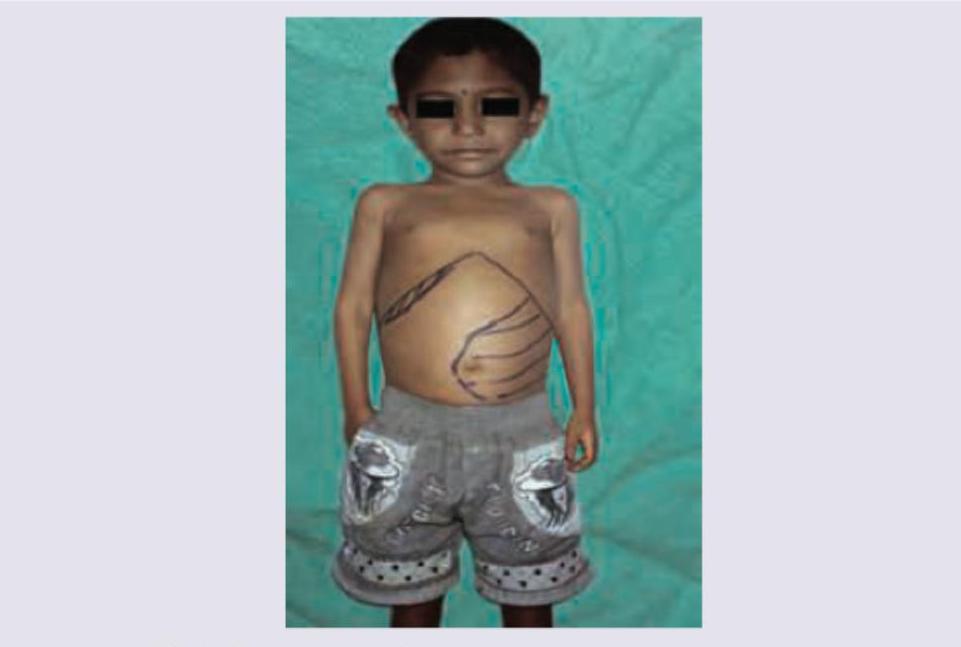
Question 10: Which of the following infections in most commonly seen in this transfusion dependant child shown below?
- A. Listeria monocytogenes
- B. Yersinia enterocolitica (Correct Answer)
- C. Acinetobacter
- D. Pneumococcus
Explanation: ***Yersinia enterocolitica*** - Transfusion-dependent patients, especially those with **iron overload** (common in thalassemia), are particularly susceptible to **Yersinia enterocolitica** infections because *Yersinia* thrives in iron-rich environments. - The image shows a child with marked hepatosplenomegaly (outlined on the abdomen), which is characteristic of conditions leading to transfusion dependence and subsequent iron overload, such as **thalassemia major**. *Listeria monocytogenes* - While *Listeria* can cause serious infections, particularly in immunocompromised individuals and neonates, its association with **iron overload** from transfusions is not as prominent as *Yersinia*. - **Listeriosis** typically presents as meningitis, sepsis, or febrile gastroenteritis. *Acinetobacter* - *Acinetobacter* species are often associated with **nosocomial infections**, affecting critically ill or immunocompromised patients in hospital settings, but not specifically linked to iron overload or transfusion dependence as a primary risk factor like *Yersinia*. - Infections commonly include pneumonia, urinary tract infections, and wound infections. *Pneumococcus* - **Pneumococcal infections** are common in children, especially those with asplenia or functional asplenia (which can occur in thalassemia due to splenic sequestration), but a direct link to **transfusion-associated iron overload** as a specific risk factor for severe pneumococcal disease is not the primary association like *Yersinia*. - These infections typically manifest as pneumonia, meningitis, and otitis media.