All SubjectsAnatomy (35)Anesthesiology (9)Biochemistry (6)Community Medicine (14)Dermatology (24)ENT (15)Forensic Medicine (18)General Medicine (22)Internal Medicine (13)Internal Medicine (5)Microbiology (25)Obstetrics and Gynecology (20)Ophthalmology (16)Orthopaedics (11)Pathology (14)Pathology (9)Pediatrics (28)Pharmacology (8)Physiology (14)Radiology (28)Surgery (4)Surgery (15)
Q11
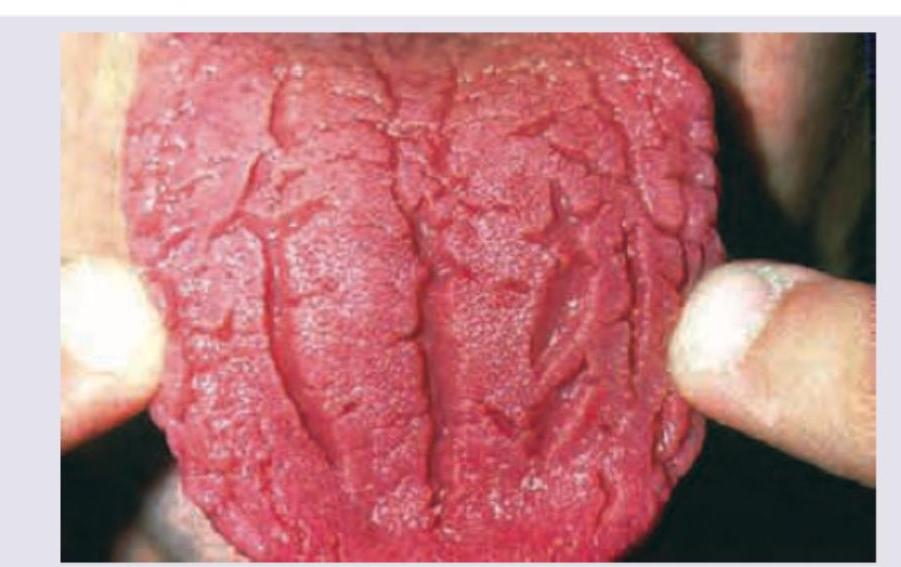
All are causes of following tongue appearance except: (Recent NEET Pattem 2016-17)
Q12
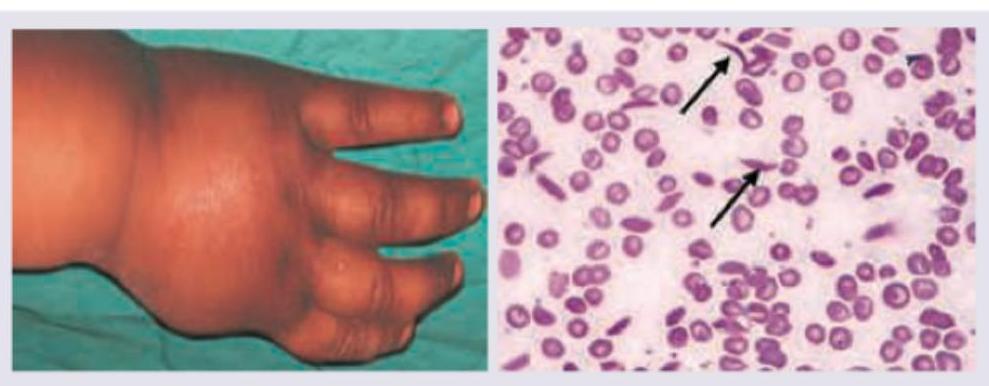
Comment on the diagnosis in the patient shown below?
Q13
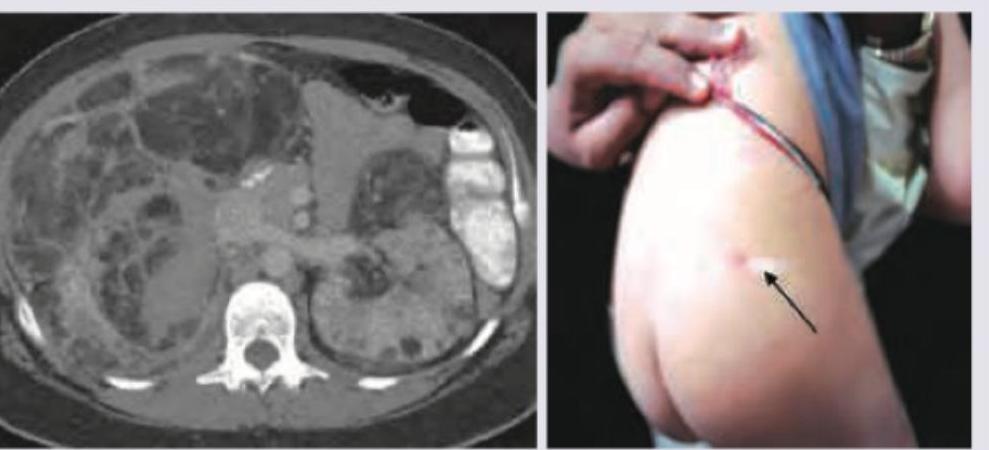
A 2-year-old mentally retarded child with the marked skin lesion presents with left side flank pain. CT scan of abdomen shows -50 to -60 HU densities of the lesions in kidney and liver. The most probable diagnosis is?
Q14
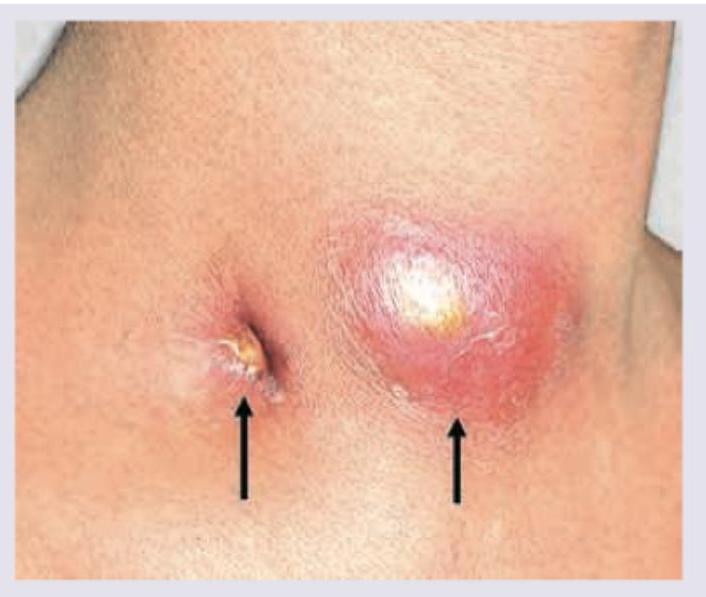
A 35-year-old HIV+ patient presents with the following lesion in the neck. What is correct about the management?
Q15
A 30-year-old AIDS patient presents with complaints as shown below. All are true about the condition except?

Q16
A 6-year-old child from Kashmir is brought to New Delhi hospital in a delirious condition with history of high grade fever for last 10 days. He is nonresponsive to commands and blanching rash is noted all over the body especially soles and palms. Per abdomen examination shows splenohepatomegaly. Probable diagnosis is:

Q17
All are correct about the organism shown in the image except: (Recent NEET Pattern 2016-17)

Q18
All are correct about the condition shown below except:

Q19
Which of the following is correct about the image shown?

Q20
A diplomat from Peru was posted to India last week. Today he has brought his 10-year-old daughter to your clinic since the child has developed this swelling in the eye and feels feverish. Comment on the clinical sign and the insect bite responsible for the same:
