NEET-PG 2017 — ENT
15 Previous Year Questions with Answers & Explanations
Which of the following is correct about ear speculum insertion?
The electrode of the hearing implant shown below is placed in:
Which of the following hearing aid or implant is shown below?
Which of the following test is being performed on the patient?

The test shown in the image is used for identifying a lesion in which cranial nerve?
MRI Brain of a 40-year-old patient with progressive unilateral SNHL and tinnitus is shown below. Which is the most common extracanalicular nerve to be involved?
A 40-year-old woman presents with history of recurrent episodes of spinning sensation in horizontal direction with vertigo incapacitating her for hours and resolving with medication. She also report roaring tinnitus during the attacks. Her sequential audiogram done on 11.06.16 and 18.06.16 is given below. Diagnosis is:
The instrument shown below is used in ENT for all except: (Recent NEET Pattern 2016-17)
All of the following statements regarding this instrument are true except: (Recent NEET Pattern 2016-17)

The facial features shown in the image are characteristic of:

NEET-PG 2017 - ENT NEET-PG Practice Questions and MCQs
Question 1: Which of the following is correct about ear speculum insertion?
- A. Pinna : upward, backward and laterally; Tragus: forward (Correct Answer)
- B. Pinna : downward, backward and laterally; Tragus: forward
- C. Pinna : upward, backward and medially; Tragus: forward
- D. Pinna : upward, forward and laterally ; Tragus: forward
Explanation: ***Pinna : upward, backward and laterally; Tragus: forward*** - To properly visualize the **tympanic membrane** and ear canal in adults, the **pinna** (auricle) should be gently pulled **upward, backward, and laterally**. This maneuver helps to straighten the **ear canal**. - The **tragus** should be gently pushed **forward** to stabilize the ear and facilitate speculum insertion, minimizing discomfort [1]. *Pinna : downward, backward and laterally; Tragus: forward* - Pulling the **pinna downward** is typically recommended for **children** to straighten their ear canal. - Doing so in adults may not adequately straighten the **ear canal**, hindering visualization. *Pinna : upward, backward and medially; Tragus: forward* - While pulling the pinna **upward and backward** is correct, pulling it **medially** would likely obstruct the view or cause discomfort. - The goal is to open the **ear canal** for better visualization [1]. *Pinna : upward, forward and laterally ; Tragus: forward* - Pulling the pinna **forward** would likely curl the helix and obstruct the **external auditory canal**, making it difficult to insert the speculum. - The correct direction is **backward** to align the cartilaginous and bony parts of the canal [1].
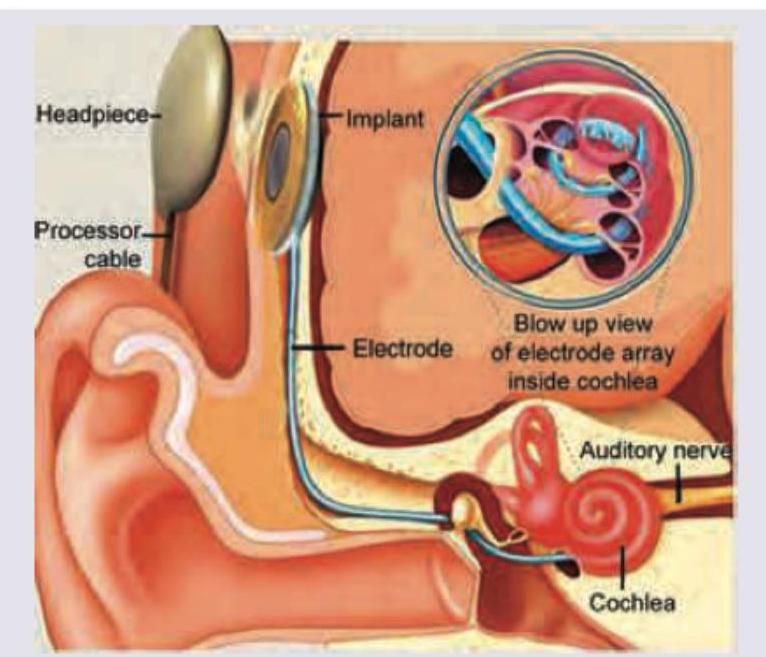
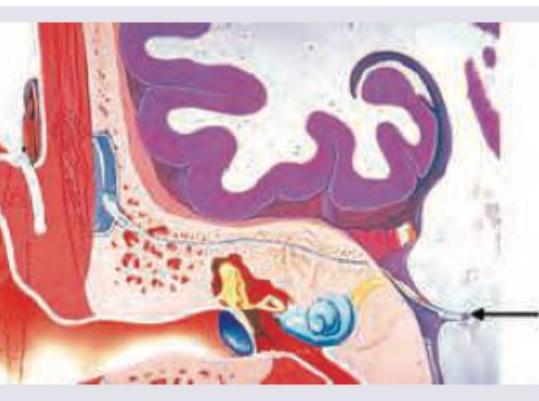
Question 2: The electrode of the hearing implant shown below is placed in:
- A. Scala vestibuli
- B. Scala tympani (Correct Answer)
- C. Scala media
- D. Tectorial membrane
Explanation: ***Scala tympani*** - The electrode array of a cochlear implant is typically inserted into the **scala tympani** to deliver electrical stimulation directly to the auditory nerve fibers. - This placement avoids damage to the delicate **organ of Corti** located in the scala media. *Scala vestibuli* - The scala vestibuli is separated from the scala media by **Reissner's membrane** and contains perilymph. - Inserting the electrode here is not the standard approach and could potentially damage the **cochlear duct**. *Scala media* - The scala media (cochlear duct) contains the **organ of Corti** and endolymph, which is crucial for natural hearing. - Placing an electrode here would likely **destroy the hair cells** and organ of Corti, preventing any residual natural hearing. *Tectorial membrane* - The tectorial membrane lies above the hair cells within the **scala media** and is essential for converting mechanical vibrations into electrical signals in natural hearing. - This membrane is not a fluid-filled space and is too delicate and structurally integral for electrode insertion.
Question 3: Which of the following hearing aid or implant is shown below?
- A. Cochlear implant (Correct Answer)
- B. Brainstem auditory implant
- C. Bone anchored hearing aid
- D. In the canal hearing aid
Explanation: ***Cochlear implant*** - The image clearly shows an **electrode array** inserted into the **cochlea**, bypassing damaged hair cells and directly stimulating the auditory nerve. - This is characteristic of a **cochlear implant**, which is used for individuals with severe to profound sensorineural hearing loss. *Brainstem auditory implant* - A **brainstem auditory implant** (BAI) electrode is placed on the **cochlear nucleus** in the brainstem, not the cochlea itself. - BAIs are typically used for conditions where the auditory nerve is damaged or absent, such as in cases of **neurofibromatosis type 2** with bilateral acoustic neuromas. *Bone anchored hearing aid* - A **bone-anchored hearing aid** (BAHA) works by transmitting sound vibrations directly to the cochlea via bone conduction, typically through a surgically implanted post or magnet in the **skull bone**. - The image does not depict an external processor or bone conduction mechanism, but rather an internal electrode within the inner ear. *In the canal hearing aid* - An **in-the-canal (ITC) hearing aid** is an external device that sits within the ear canal and amplifies sound acoustically. - The image shows an **invasive internal device** implanted into the cochlea, which is distinct from a non-invasive, external ITC hearing aid.
Question 4: Which of the following test is being performed on the patient?
- A. Caloric stimulation test
- B. Doll's eye reflex
- C. Dix-Hallpike test (Correct Answer)
- D. Frenzel maneuver
Explanation: ***Dix-Hallpike test*** - The image depicts a patient being moved from an upright sitting position to a supine position with the head turned to one side and extended, which is characteristic of the **Dix-Hallpike maneuver**. - This test is used to diagnose **benign paroxysmal positional vertigo (BPPV)** by provoking vertigo and nystagmus as a result of otoconia displacement in the semicircular canals. *Caloric stimulation test* - This test involves introducing **warm or cold water/air into the ear canal** to induce nystagmus, assessing the vestibular system. - It's typically performed with the patient lying supine with their head elevated at 30 degrees, not involving the specific positional changes shown in the image. *Doll's eye reflex* - Also known as the **oculocephalic reflex**, it assesses brainstem function by rapidly turning the patient's head while observing eye movement. - This reflex is primarily used to evaluate comatose patients and does not involve the complex body and head positioning seen in the image. *Frenzel maneuver* - The Frenzel maneuver is performed during **otoscopy** to check for nystagmus by having the patient gaze through high plus lenses in a dark room. - It is often used to suppress visual fixation and enhance nystagmus, but it does not involve the specific body or head movements depicted.
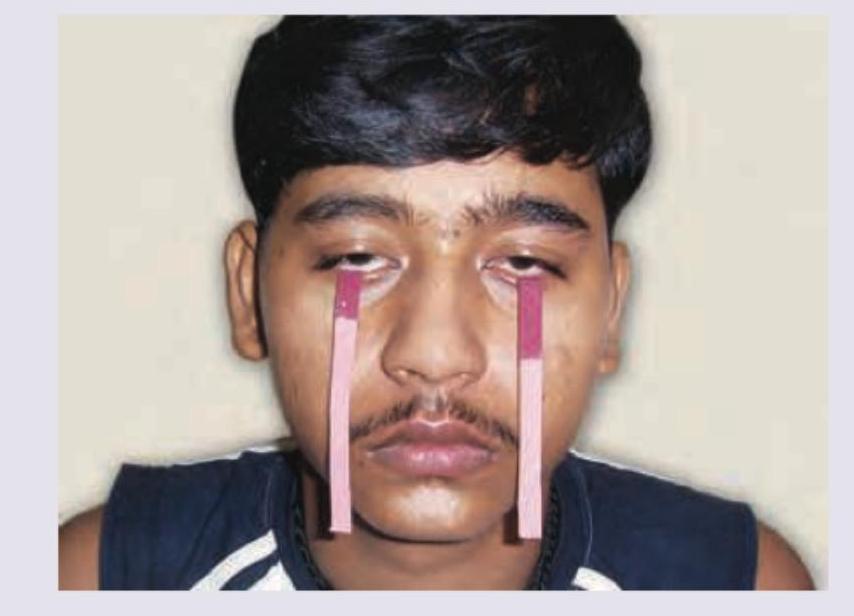
Question 5: The test shown in the image is used for identifying a lesion in which cranial nerve?
- A. III
- B. VI
- C. VII (Correct Answer)
- D. VIII
Explanation: ***VII*** - The image shows a **Schirmer's test** being conducted, which measures **tear production**. - Tear production is primarily innervated by the **facial nerve (cranial nerve VII)**, making this test relevant for evaluating its function related to lacrimation. *III* - Cranial nerve III (oculomotor nerve) controls most **extraocular muscles**, pupillary constriction, and lid elevation. A lesion would manifest as issues with eye movement, ptosis, or pupil dilation, not tear production. - The Schirmer's test does not directly assess the function of the **oculomotor nerve**. *VI* - Cranial nerve VI (abducens nerve) innervates the **lateral rectus muscle**, responsible for abducting the eye (moving it outwards). - A lesion in CN VI would cause **diplopia** and inability to move the eye laterally, which is unrelated to tear production. *VIII* - Cranial nerve VIII (vestibulocochlear nerve) is responsible for **hearing** and **balance**. - Lesions affect hearing (e.g., deafness, tinnitus) or balance (e.g., vertigo, nystagmus), and have no direct involvement in tear production.
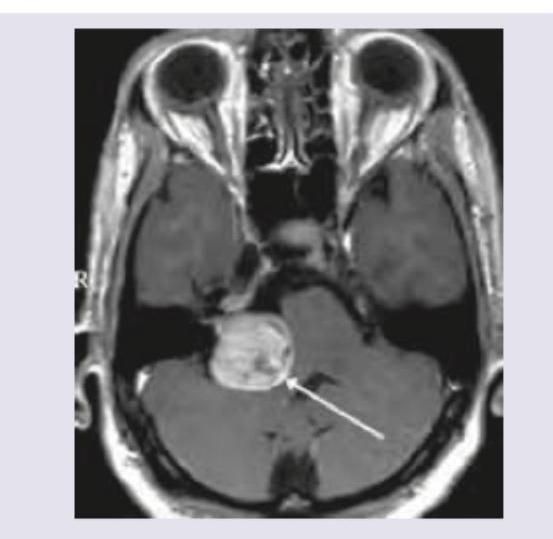
Question 6: MRI Brain of a 40-year-old patient with progressive unilateral SNHL and tinnitus is shown below. Which is the most common extracanalicular nerve to be involved?
- A. V (Correct Answer)
- B. VI
- C. VII
- D. VIII
Explanation: ***V*** - The image shows a large **right cerebellopontine angle (CPA) mass**, consistent with an **acoustic neuroma** (vestibular schwannoma), which commonly arises from CN VIII in the internal auditory canal and extends into the CPA. - The **trigeminal nerve (CN V)** is the most common extracanalicular cranial nerve to be compressed and involved by larger CPA tumors due to its proximity and superior-anterior position relative to CN VIII. *VI* - The abducens nerve (CN VI) controls the lateral rectus muscle of the eye, and its involvement typically causes **diplopia** and **lateral gaze palsy**. While possible with very large and medially extending CPA tumors, it is less common than CN V involvement. - CN VI is located more medially and anteriorly within the brainstem and generally requires significant mass effect rather than direct compression from a typical CPA tumor. *VII* - The facial nerve (CN VII) travels with the vestibulocochlear nerve (CN VIII) through the **internal auditory canal**, and is frequently involved by acoustic neuromas within the canal, leading to **facial weakness or paralysis**. - However, the question specifically asks for the most common **extracanalicular** nerve involvement. While CN VII is intimately associated, its most common site of involvement is within the canal, or early in the CPA, and V is often implicated with larger CPA masses. *VIII* - The vestibulocochlear nerve (CN VIII) is the nerve from which **acoustic neuromas (vestibular schwannomas)** originate, causing the presenting symptoms of **unilateral SNHL and tinnitus**. Therefore, it is the primary affected nerve, not an extracanalicular one involved due to compression. - The question asks for the most common **extracanalicular nerve to be involved**, implying a nerve *other than* the one the tumor originates from or primarily affects locally within the canal.
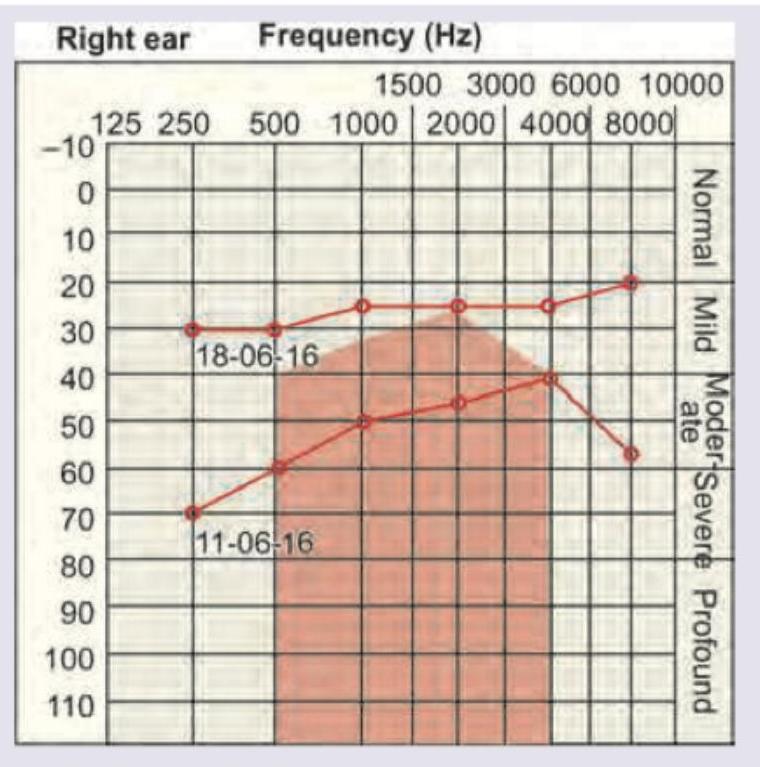
Question 7: A 40-year-old woman presents with history of recurrent episodes of spinning sensation in horizontal direction with vertigo incapacitating her for hours and resolving with medication. She also report roaring tinnitus during the attacks. Her sequential audiogram done on 11.06.16 and 18.06.16 is given below. Diagnosis is:
- A. Migraine variant
- B. Benign paroxysmal positional vertigo
- C. Acoustic neuroma
- D. Meniere's disease (Correct Answer)
Explanation: ### ***Meniere's disease*** - This patient presents with the classic triad of **Meniere's disease**: recurrent **vertigo**, **roaring tinnitus**, and fluctuating **sensorineural hearing loss** (as shown by the sequential audiograms with improvement). - The audiogram demonstrates **fluctuating hearing loss**, which is typical for Meniere's, with the hearing loss being worse on June 11th and improving by June 18th, particularly at lower frequencies (a pattern often seen in Meniere's). ### *Migraine variant* - While migraine can cause vertigo (**vestibular migraine**), it typically does not present with characteristic **roaring tinnitus** or **fluctuating hearing loss** on audiometry. - The audiogram showing a clear pattern of fluctuating sensorineural hearing loss points away from an isolated migraine variant. ### *Benign paroxysmal positional vertigo* - BPPV causes **brief episodes of vertigo** triggered by specific head movements, usually lasting seconds to a minute, and is not associated with roaring tinnitus or hearing loss. - The patient's vertigo episodes are described as "incapacitating her for hours," which is inconsistent with the short duration of BPPV attacks. ### *Acoustic neuroma* - An acoustic neuroma typically causes **progressive, unilateral sensorineural hearing loss**, persistent tinnitus (often high-pitched), and sometimes imbalance, but **recurrent, sudden, severe vertigo** and **fluctuating hearing** are less common. - The rapid fluctuation and improvement in hearing shown on the sequential audiograms are not characteristic of the generally slow, progressive nature of hearing loss due to an acoustic neuroma.
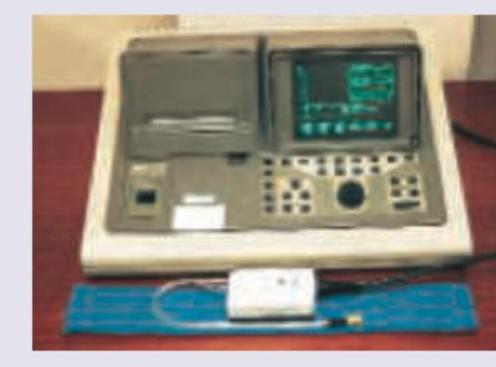
Question 8: The instrument shown below is used in ENT for all except: (Recent NEET Pattern 2016-17)
- A. Status of middle ear
- B. Status of tympanic membrane
- C. Acoustic reflex
- D. Oculovestibular reflex (Correct Answer)
Explanation: ***Oculovestibular reflex*** - The image shows a **tympanometer**, which is used to assess the function of the middle ear and Eustachian tube through **impedance audiometry**. - The **oculovestibular reflex** (also known as the **caloric reflex test**) assesses the function of the vestibular system and brainstem using cold or warm water/air irrigation of the ear canal, and is **not evaluated by tympanometry**. - This is the correct answer as it is the only function NOT assessed by the tympanometer. *Status of middle ear* - Tympanometry directly measures the **compliance of the tympanic membrane** and the **pressure in the middle ear space**, providing information about middle ear pathologies. - It can help diagnose conditions like **otitis media with effusion**, **eustachian tube dysfunction**, and **otosclerosis** by analyzing the tympanogram shape (Type A, B, C, etc.). *Status of tympanic membrane* - Tympanometry measures how the **tympanic membrane moves in response to changes in air pressure** in the external ear canal. - This movement pattern, depicted in the tympanogram, indicates the **flexibility and integrity of the tympanic membrane**. *Acoustic reflex* - The **acoustic reflex (stapedial reflex)** CAN be measured using **impedance audiometry**, which includes the tympanometer. - When a loud sound (70-100 dB above hearing threshold) is presented, the stapedius muscle contracts, causing a change in middle ear impedance that is detected by the tympanometer. - This reflex tests the integrity of the **auditory pathway from CN VIII through the brainstem to CN VII**, and is useful in diagnosing conditions like **acoustic neuroma**, **facial nerve palsy**, and **cochlear vs retrocochlear pathology**.
Question 9: All of the following statements regarding this instrument are true except: (Recent NEET Pattern 2016-17)
- A. Speculum that is used here has a concave lens with a magnification of 2.5 times
- B. This device is used to assess tympanic membrane mobility
- C. This device is used to suck out middle ear secretions
- D. This device is used to administer antibiotics in the middle ear cavity (Correct Answer)
Explanation: ***This device is used to administer antibiotics in the middle ear cavity*** - The image shows a **Pneumatic Otoscope**, which is primarily used for **diagnostic purposes**, specifically to assess tympanic membrane mobility, not for administering medications. - Administering antibiotics directly into the middle ear typically requires more invasive procedures like **myringotomy** with ear tube placement, or direct injection, which are not performed with this device. *Speculum that is used here has a concave lens with a magnification of 2.5 times* - The otoscope head has a **magnifying lens**, typically around **2.5x**, to allow for clearer visualization of the ear canal and tympanic membrane. - While it has a magnifying lens, stating it's a **concave lens** is generally incorrect in the context of an otoscope's primary magnifying lens, which is typically a **convex lens** for magnification. *This device is used to access tympanic membrane mobility* - The rubber bulb and tubing attached to the otoscope are designed to create **positive and negative air pressure** within the external ear canal. - This pressure change allows the clinician to observe the **movement (mobility)** of the tympanic membrane, which is crucial for diagnosing conditions like **otitis media with effusion**. *This device is used to suck out middle ear secretions* - While otoscopes can be used to visualize secretions in the external ear canal or visible through a perforated tympanic membrane, this particular device is not designed for **suctioning middle ear secretions**. - Suctioning middle ear secretions would typically require a **surgical microscope** and specialized **suction instruments** or a **myringotomy** procedure.
Question 10: The facial features shown in the image are characteristic of:
- A. Frog face deformity
- B. Adenoid facies (Correct Answer)
- C. Ashen grey facies
- D. Thyrotoxicosis
Explanation: ***Adenoid facies*** - The image displays characteristic features of adenoid facies, including a **long, open-mouthed face**, a **pinched nose**, and possibly a **high-arched palate** due to chronic mouth breathing from enlarged adenoids. - This chronic condition often leads to a dull expression, sometimes with **strabismus** (crossed eyes) as seen in the image, and a forward head posture. *Frog face deformity* - This deformity is characterized by **ocular hypertelorism** (widely spaced eyes), a **flat nasal bridge**, and a **short nose**, often associated with conditions like Apert syndrome. - While there is some facial dysmorphology, the specific combination of features does not align with a typical frog face. *Ashen grey facies* - This refers to a **pale, grayish complexion**, often indicative of severe cardiovascular compromise like **circulatory collapse** or **shock**. - The child in the image has a normal skin tone for their ethnicity and does not show signs of acute circulatory distress. *Thyrotoxicosis* - **Thyrotoxicosis** (hyperthyroidism) in children can cause symptoms like **exophthalmos** (bulging eyes), **tachycardia**, weight loss, and an enlarged thyroid gland. - While the child's eyes appear wide-set and sometimes strabismic, these are more consistent with the long-term effects of chronic mouth breathing on facial development rather than acute thyroid dysfunction.