All SubjectsAnatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q21
A 41-year-old male complains of itching on the upper chest for one month. What is the most likely diagnosis?

Q22
A patient presents with intensely pruritic vesicular lesions on extensor surfaces. What is the most likely diagnosis based on the clinical image?

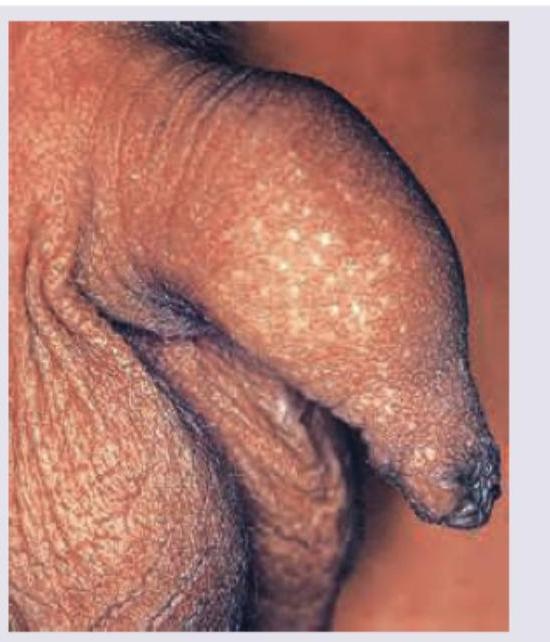
Q23
A 20-year-old male with no history of any sexual contact presents with following lesions on his penis. What is the diagnosis?
Q24
What is the most likely diagnosis of the image given below?
