All SubjectsAnatomy (30)Anesthesiology (8)Biochemistry (8)Community Medicine (17)Dermatology (24)ENT (18)Forensic Medicine (18)General Medicine (2)Internal Medicine (23)Internal Medicine (8)Microbiology (39)Obstetrics and Gynecology (15)Ophthalmology (16)Orthopaedics (11)Pathology (10)Pathology (17)Pediatrics (26)Pharmacology (6)Physiology (15)Radiology (30)Surgery (5)Surgery (22)
Q11
A 25-year-old construction worker presents with following skin lesions. All are true about the image shown except: (Recent NEET Pattern 2016-17)

Q12
A 1-year-old unimmunised child with HbsAg positivity is having following skin lesions. What is the diagnosis?

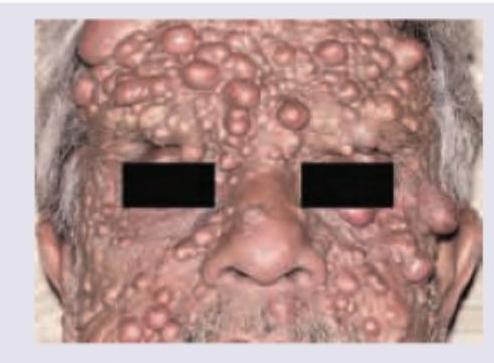
Q13
Identify the lesion shown in the image:

Q14
A 13-year-old boy presents with patchy depigmented skin on the right flank and upper thigh in segmental distribution, as shown in the image. The depigmentation started 1 year back but has been static for last 4 months. Mother reports use of topical steroids which was ineffective. Diagnosis is?

Q15
What is the diagnosis based on the clinical image shown?
Q16
What is the most likely diagnosis of the image provided below?

Q17
A patient presents with oral mucosal lesions. Identify the condition shown in the image:

Q18
Identify the lesion:

Q19
Identify the lesion:

Q20
A patient presents with violaceous papules over the knuckles and mottled pigmentation on the dorsum of hands. Identify the lesion:
