NEET-PG 2017 — Anesthesiology
9 Previous Year Questions with Answers & Explanations
All are correct about the pressure recording shown below except: (Recent NEET Pattern 2016-17)
Which of the knobs shown below represent the knob controlling oxygen flow in the anesthesia machine?
What ventilation modality is shown below?
Which of the following Mapleson system is shown below?
What does the following capnographic recording represent?
All are complications of this anesthesia technique except: (Recent NEET Pattern 2016-17)

All are contraindications of this anesthesia technique except: (Recent NEET Pattern 2016-17)
Which finding indicates correct placement of needle in this nerve block? (Recent NEET Pattern 2016-17)
Which is correct about the anesthetic drugs X and Y in the image shown? (Recent NEET Pattern 2016-17)
NEET-PG 2017 - Anesthesiology NEET-PG Practice Questions and MCQs
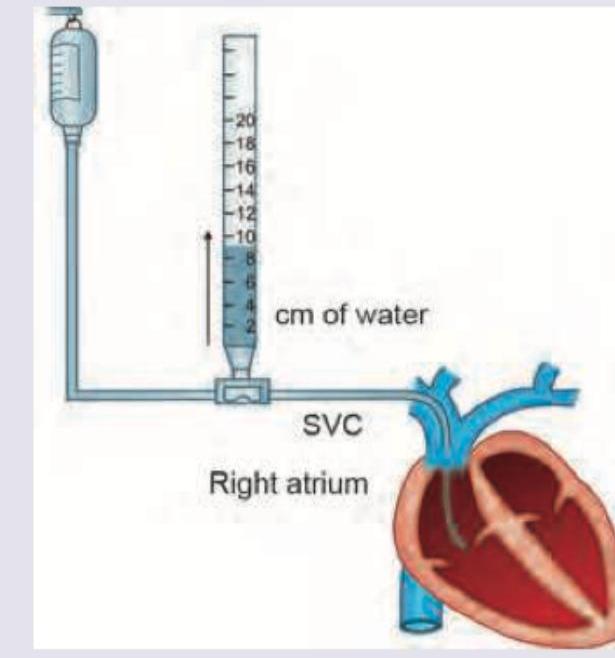
Question 1: All are correct about the pressure recording shown below except: (Recent NEET Pattern 2016-17)
- A. Normal CVP is 2-10 cm of water
- B. Pressure recording of more than 10 cm of water implies restricting IV fluids to the patient
- C. Venous catheter is advanced into subclavicular IVC
- D. Can be used to assess left ventricular function (Correct Answer)
Explanation: ***Can be used to assess left ventricular function*** - Central venous pressure (CVP) primarily reflects **right atrial pressure** and, indirectly, **right ventricular end-diastolic pressure**. - It is **not a reliable indicator** for assessing **left ventricular function**, which is better gauged by pulmonary artery wedge pressure (PAWP) or echocardiography. *Normal CVP is 2-10 cm of water* - The image depicts a manometer measuring CVP in **cm of water**. - The generally accepted normal range for CVP is **2-10 cm H2O** (or 0-8 mmHg), reflecting adequate right heart filling and venous return. *Pressure recording of more than 10 cm of water implies restricting IV fluids to the patient* - A CVP **above 10 cm H2O** (or 8 mmHg) typically indicates **fluid overload**, increased right ventricular preload, or right ventricular dysfunction. - In such cases, **restricting intravenous fluids** is often appropriate to prevent further circulatory congestion and potential complications like pulmonary edema. *Venous catheter is advanced into subclavicular IVC* - For CVP measurement, the catheter tip should ideally be positioned in the **superior vena cava (SVC)**, near its junction with the **right atrium**. - Advancing the catheter into the **inferior vena cava (IVC)** is anatomically incorrect for standard CVP measurement, as it would not reflect right atrial pressure as directly or accurately.
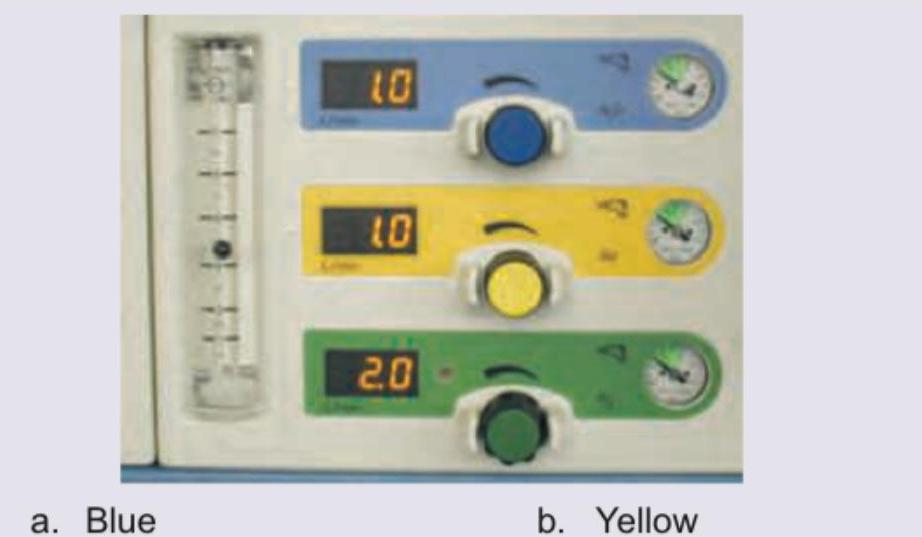
Question 2: Which of the knobs shown below represent the knob controlling oxygen flow in the anesthesia machine?
- A. Blue (Correct Answer)
- B. Yellow
- C. Green
- D. None
Explanation: ***Blue*** - In anesthesia machines, the blue knob typically controls the flow of **nitrous oxide**. However, in the provided image, the blue knob is labeled with "O2" (implied by the digital display indicating "10" which typically refers to **liters per minute of oxygen**). The question asks for the knob controlling oxygen flow, and based on the provided image, the blue knob corresponds to oxygen. - The digital display next to the blue knob reads "10", which in the context of anesthesia machines, usually signifies a flow rate in **liters per minute**. Given that the question asks for the oxygen flow control, and it is common for oxygen to be blue-coded in some parts of the world, this is the most logical choice depicted. *Yellow* - The yellow knob is labeled "Air" (implied by the digital display indicating "10"). This knob would control the flow of **medical air**, not oxygen. - Medical air is a distinct gas from oxygen, used for different purposes in anesthesia. *Green* - The green knob is labeled "N2O," representing **nitrous oxide**. This knob controls the flow of nitrous oxide, which is an anesthetic gas. - Nitrous oxide is typically color-coded blue in some regions (like the US) but green in others (like the UK/Europe), similar to how oxygen can be white or green. However, in this specific image, green is clearly labeled N2O. *None* - This option is incorrect because the image clearly shows a knob, specifically the blue one, designated for oxygen flow (implied by the "O2" display). - The presence of color-coded knobs with corresponding digital displays for gas flow negates the possibility of "None" being the correct answer.
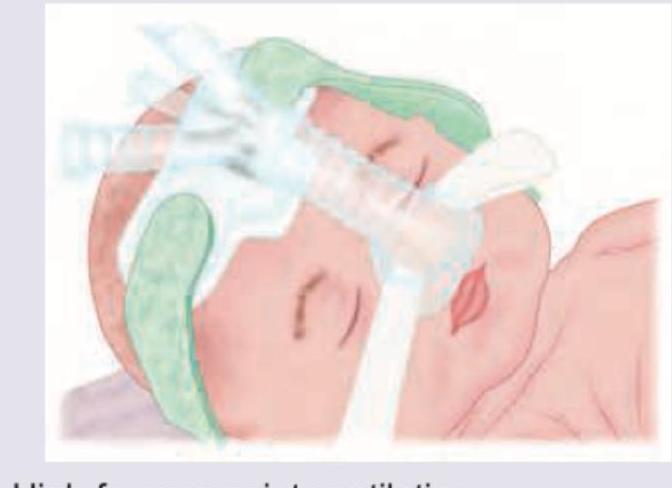
Question 3: What ventilation modality is shown below?
- A. High frequency jet ventilation
- B. Nasal CPAP (Correct Answer)
- C. Inverse ratio ventilation
- D. Intermittent positive pressure ventilation
Explanation: ***Nasal CPAP*** - The image shows a device applied to the nose of an infant, providing a continuous flow of air which is characteristic of **Nasal Continuous Positive Airway Pressure (nCPAP)**. - This modality helps maintain lung volume, improve oxygenation, and reduce the work of breathing in neonates with respiratory distress. *High frequency jet ventilation* - This modality involves delivering small tidal volumes at very **high frequencies** (hundreds of breaths per minute) through a specialized ventilator and endotracheal tube. - The image does not depict an **endotracheal tube** or the rapid, small tidal volume delivery characteristic of jet ventilation. *Inverse ratio ventilation* - This is a mode of **mechanical ventilation** where the inspiratory time is longer than the expiratory time (I:E ratio > 1:1), typically used in intubated patients. - The image shows a non-invasive nasal device, not an **intubated patient** on a mechanical ventilator. *Intermittent positive pressure ventilation* - This refers to delivering breaths with positive pressure, either invasively (via endotracheal tube) or non-invasively (via mask), to assist or control breathing. - While CPAP provides positive pressure, "intermittent positive pressure ventilation" implies cyclical breaths, which is not the primary defining feature shown, and CPAP (continuous pressure) is a more specific and accurate description for the depicted setup.
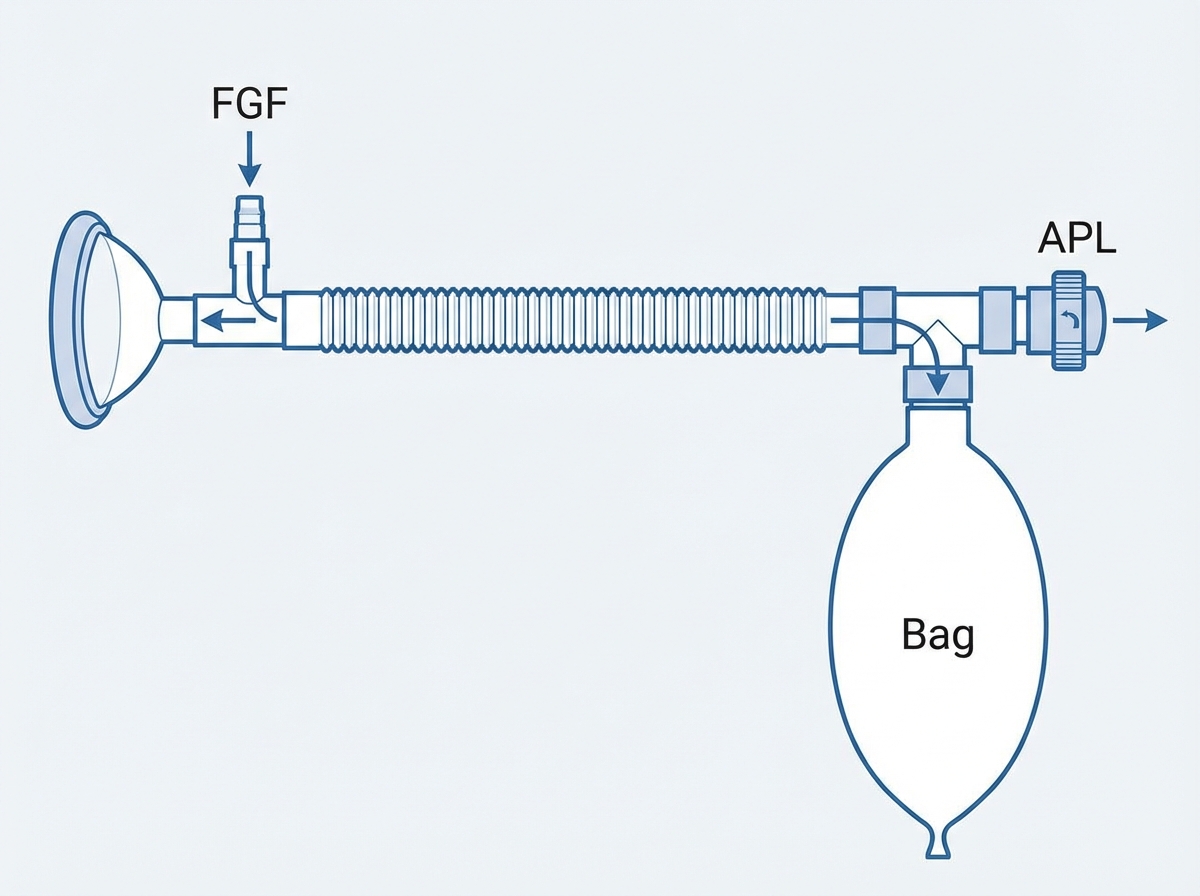
Question 4: Which of the following Mapleson system is shown below?
- A. Mapleson C
- B. Mapleson A
- C. Mapleson B
- D. Mapleson D (Correct Answer)
Explanation: ***Mapleson D*** - This system is characterized by the **fresh gas inlet (FG)** being close to the patient end (P) and the **reservoir bag** and **adjustable pressure-limiting (APL) valve (T)** being further away, typically near the expiratory limb. The corrugated tube separates the bag and valve from the patient. - The image clearly depicts the **fresh gas entering near a reservoir bag**, which is then connected via a corrugated tube to the patient end, with an **APL valve (T)** situated near the patient, right before the patient connection, which is characteristic of the Mapleson D system. *Mapleson A* - In a Mapleson A system, the **fresh gas inlet** is located near the **reservoir bag**, which is positioned far from the patient. The APL valve is also near the reservoir bag. - This arrangement is highly efficient for **spontaneous ventilation** but less so for controlled ventilation. The image shows a different configuration. *Mapleson B* - The Mapleson B system has both the **fresh gas inlet** and the **APL valve** close to the patient, with the reservoir bag at the end of a long expiratory limb. - This system is **not very efficient** for either spontaneous or controlled ventilation due to significant rebreathing potential, which is unlike the depicted system. *Mapleson C* - This system is similar to Mapleson B but with a **shorter expiratory limb**, making it more compact. - Both the **fresh gas inlet** and the **APL valve** are near the patient, with the reservoir bag also close to the patient. The image clearly shows a long corrugated tube, making this option incorrect.
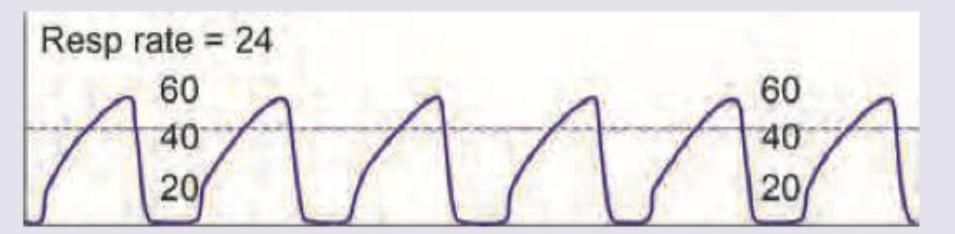
Question 5: What does the following capnographic recording represent?
- A. Asthma (Correct Answer)
- B. Spontaneous extubation
- C. Raised ICT
- D. Air embolism
Explanation: ***Asthma*** - The capnographic tracing shows a characteristic **shark fin waveform**, indicative of **expiratory airflow obstruction**. - This waveform is generated due to uneven emptying of the alveoli, where CO2 continues to be exhaled at a reduced rate during the later phase of expiration. *Spontaneous extubation* - Spontaneous extubation would typically result in a **complete loss of the capnography waveform** due to disconnection from the airway. - The tracing shown still clearly depicts expired CO2, inconsistent with complete extubation. *Raised ICT* - Raised intracranial tension (ICT) can affect breathing patterns (e.g., Cheyne-Stokes, hyperventilation), but it does not directly produce a a **shark fin capnography waveform**. - Capnography reflects CO2 elimination, which can be indirectly affected by changes in ventilatory drive from raised ICT but not in this specific shape. *Air embolism* - An air embolism would cause a sudden **drop in end-tidal CO2 (EtCO2)**, often to zero, due to obstruction of pulmonary blood flow, leading to alveolar dead space. - The waveform shown does not depict a sudden drop to zero or significantly reduced EtCO2.
Question 6: All are complications of this anesthesia technique except: (Recent NEET Pattern 2016-17)
- A. Bradycardia
- B. Sudden cardiac arrest
- C. Decrease in vital capacity
- D. Paralytic ileus (Correct Answer)
Explanation: **SPINAL ANESTHESIA COMPLICATIONS ANALYSIS:** ***Paralytic ileus*** - While spinal anesthesia can cause some **decreased bowel motility** due to sympathetic blockade, true **paralytic ileus** is primarily associated with **abdominal surgery**, **prolonged opioid use**, **electrolyte imbalances**, or **systemic illness**. - **Paralytic ileus** is not considered a direct complication of spinal anesthesia technique itself, making it the exception among the given options. *Bradycardia* - Direct result of **sympathetic blockade** affecting **cardiac accelerator fibers**, leading to unopposed **vagal activity**. - Common complication of spinal anesthesia due to blocked sympathetic innervation that normally maintains heart rate. *Sudden cardiac arrest* - Rare but serious complication from severe **bradycardia** and **hypotension**, especially with **high spinal blocks**. - Can occur when sympathetic blockade extends too high, affecting critical **cardiovascular control mechanisms**. *Decrease in vital capacity* - Results from **motor blockade** of **intercostal muscles** and potentially **phrenic nerve** with high spinal blocks. - Respiratory compromise can be significant, particularly in patients with pre-existing **pulmonary disease**. **Conclusion:** Paralytic ileus is the exception as it is not a direct complication of spinal anesthesia, unlike the other cardiovascular and respiratory complications listed.
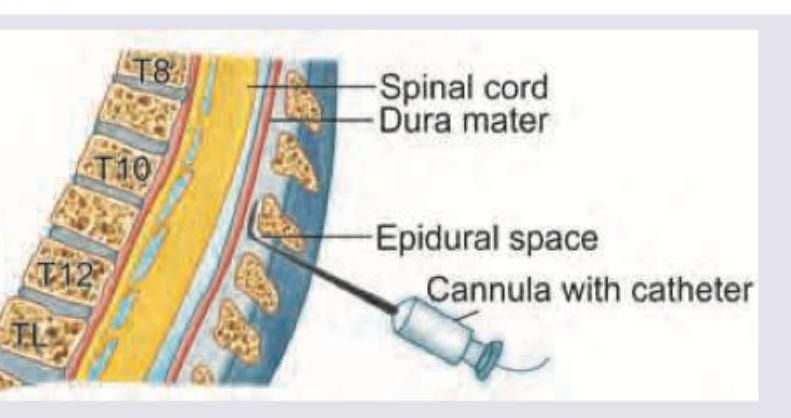
Question 7: All are contraindications of this anesthesia technique except: (Recent NEET Pattern 2016-17)
- A. Bleeding diathesis
- B. Severe aortic stenosis
- C. Aortic aneurysm (Correct Answer)
- D. Uncooperative patient
Explanation: ***Aortic aneurysm*** - An **aortic aneurysm** is not a contraindication for **epidural anesthesia**. In fact, epidural anesthesia can be beneficial for patients with aortic aneurysms during surgical repair as it can help stabilize hemodynamics and provide effective pain control. - The image shows a needle entering the **epidural space**, indicating this question pertains to epidural anesthesia. *Bleeding diathesis* - **Bleeding diathesis** is a **relative contraindication** for **epidural anesthesia** due to the increased risk of **epidural hematoma**, which can cause neurological damage. - The formation of an **epidural hematoma** can lead to spinal cord compression. *Severe aortic stenosis* - **Severe aortic stenosis** is a **contraindication** for **epidural anesthesia** because the associated **vasodilation** from regional anesthesia can lead to a drastic drop in blood pressure, which these patients cannot tolerate as their fixed cardiac output relies on adequate preload. - Patients with **severe aortic stenosis** are highly susceptible to **hypotension** and cardiac collapse. *Uncooperative patient* - An **uncooperative patient** is a **contraindication** for **epidural anesthesia** as proper positioning and patient cooperation are crucial for safe needle placement. - Lack of cooperation increases the risk of **neurological injury** during the procedure.
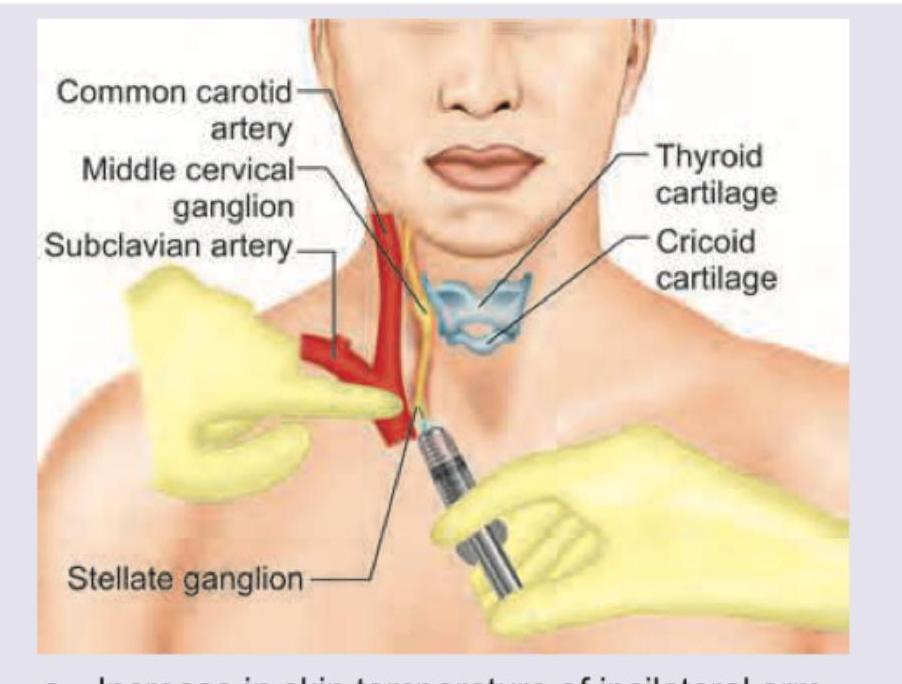
Question 8: Which finding indicates correct placement of needle in this nerve block? (Recent NEET Pattern 2016-17)
- A. Increase in skin temperature of ipsilateral arm (Correct Answer)
- B. Decrease in skin temperature of ipsilateral arm
- C. Increase in sweating of ipsilateral arm
- D. Decrease in sweating of ipsilateral arm
Explanation: ***Increase in skin temperature of ipsilateral arm*** - A successful **stellate ganglion block** interrupts the **sympathetic efferent fibers** that innervate the ipsilateral arm. - This interruption leads to **vasodilation** in the blood vessels of the arm, resulting in increased blood flow and thus, a rise in skin temperature. *Decrease in skin temperature of ipsilateral arm* - A decrease in skin temperature would indicate **vasoconstriction**, which is the opposite effect of a successful sympathetic block. - This would suggest either an ineffective block or stimulation of sympathetic activity. *Increase in sweating of ipsilateral arm* - The stellate ganglion also carries **sympathetic fibers** to the sweat glands. A successful block would inhibit sweat gland activity. - Increased sweating (known as **diaphoresis**) would indicate an inadequate block or irritation of the ganglion, leading to increased sympathetic outflow. *Decrease in sweating of ipsilateral arm* - While a **decrease in sweating** (anhidrosis) is indeed a sign of effective sympathetic blockade to the arm, it is typically less immediate and less clinically observable than the change in skin temperature. - The most easily and consistently observed sign of sympathetic denervation in the arm is the increase in skin temperature due to vasodilation.
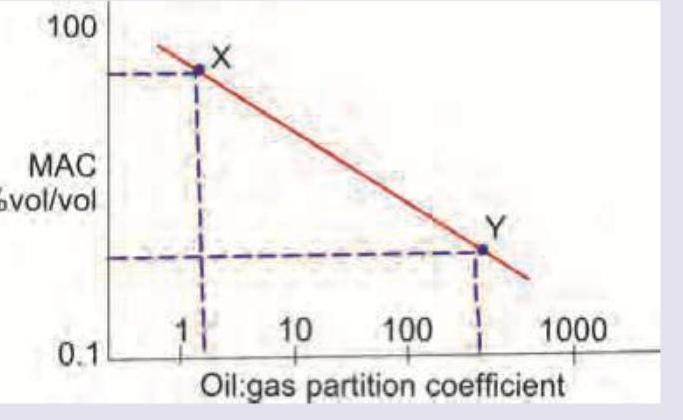
Question 9: Which is correct about the anesthetic drugs X and Y in the image shown? (Recent NEET Pattern 2016-17)
- A. Drug X and Y have equally fast onset of action
- B. Drug X and Y have equally fast onset of action but potency of X is more than Y
- C. Drug Y is more fast acting than X
- D. Drug X is more fast acting than Y (Correct Answer)
Explanation: ***Drug X is more fast acting than Y*** - The **oil:gas partition coefficient** for Drug X is lower than for Drug Y. A lower oil:gas partition coefficient typically correlates with a **faster onset of action** for inhaled anesthetics as it indicates lower solubility in blood and tissues, allowing for quicker equilibration in the brain. - While MAC is plotted against oil:gas partition coefficient, the question specifically asks about **onset of action**, which is primarily influenced by blood-gas solubility rather than oil-gas solubility. However, an anesthetic with lower oil-gas solubility (like X) would generally also have lower blood-gas solubility, leading to faster onset. *Drug Y is more fast acting than X* - Drug Y has a **higher oil:gas partition coefficient** compared to Drug X, indicating greater lipid solubility. - A higher oil:gas partition coefficient generally correlates with a **slower onset of action** for inhaled anesthetics, as more drug dissolves in lipids before reaching the brain. *Drug X and Y have equally fast onset of action* - The graph clearly shows that Drug X and Drug Y have different **oil:gas partition coefficients**. - Since the partition coefficients are different, their **solubility characteristics** and therefore their clinical onset of action would also be different. *Drug X and Y have equally fast onset of action but potency of X is more than Y* - Onset of action is **not equal** for X and Y due to their differing oil:gas partition coefficients. - Potency, represented by **MAC** (Minimum Alveolar Concentration), is inversely related to the oil:gas partition coefficient for many inhaled anesthetics. From the graph, Drug X has a higher MAC value than Drug Y (meaning it is **less potent** but acts faster).