NEET-PG 2017 — Anatomy
35 Previous Year Questions with Answers & Explanations
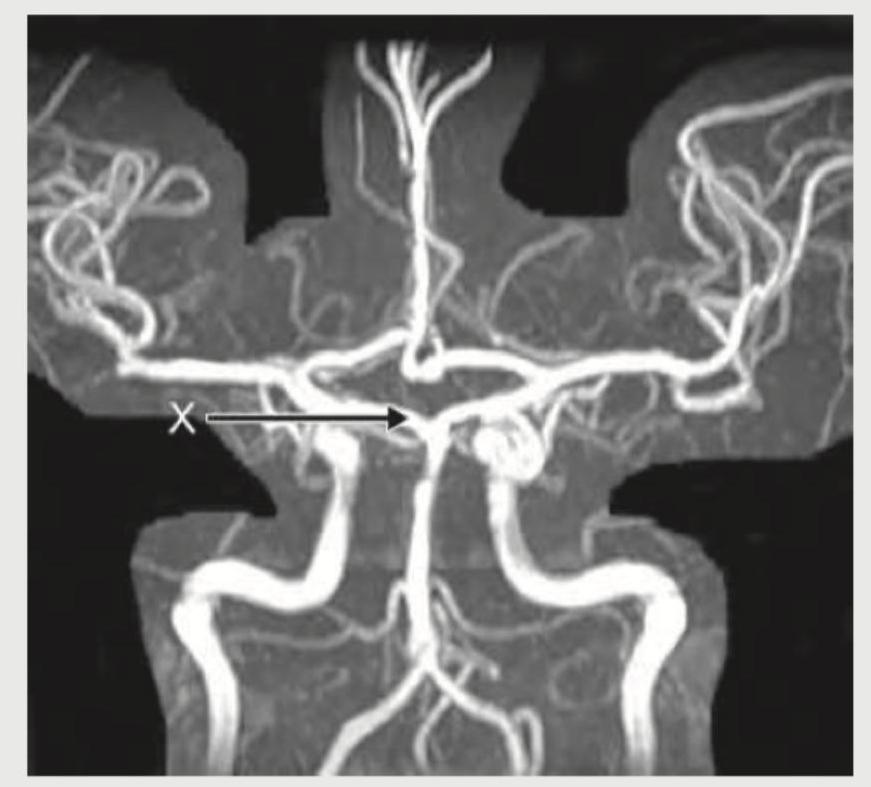
What is the name of the marked blood vessel shown in brain circulation?

What is the name of the marked blood vessel in the Circle of Willis?
All of the following layers are pierced by the needle shown below except:

All investigations are useful in work up of this condition except:

A 2-day-old neonate under phototherapy unit. For exchange transfusion serum bilirubin-albumin ratio should be: (Recent NEET Pattern 2016-17)
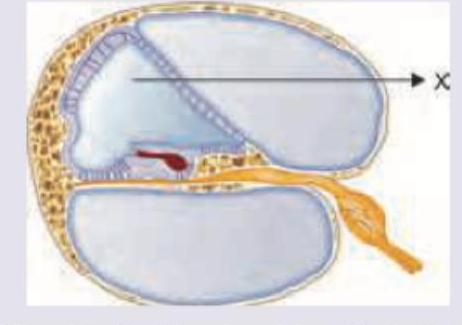
What is correct about the composition of fluid in the area marked as $X$ ?
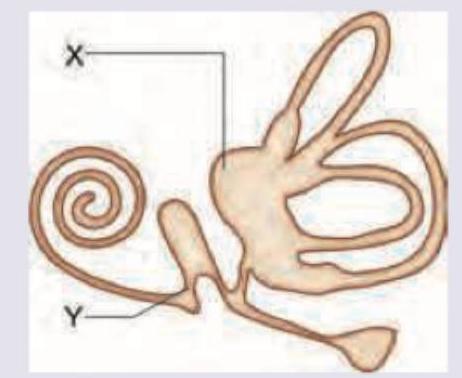
All are correct about the part marked as $X$ and $Y$ except:
All are true about the terminal area marked 'X' in this bacteria except:

Which of the following is correct about the image shown?
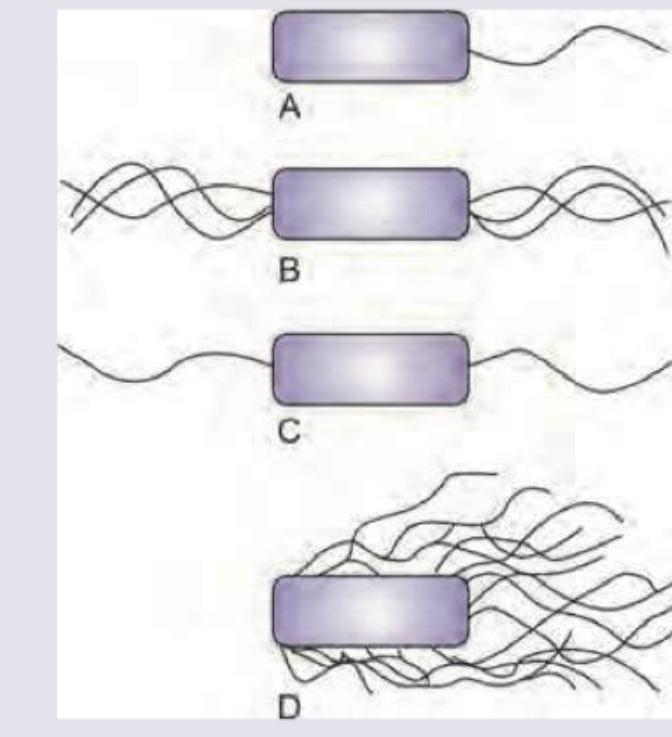
Which of the following bacteria will have following appearance?
NEET-PG 2017 - Anatomy NEET-PG Practice Questions and MCQs
Question 1: What is the name of the marked blood vessel shown in brain circulation?
- A. Middle cerebral artery
- B. Posterior communicating artery (Correct Answer)
- C. Internal carotid artery
- D. Anterior communicating artery
Explanation: ***Posterior communicating artery*** - The arrow points to a vessel connecting the **anterior circulation** (internal carotid artery system) with the **posterior circulation** (vertebrobasilar system) within the **Circle of Willis**. - This specific location and function are characteristic of the **posterior communicating artery**, which typically arises from the internal carotid and joins the posterior cerebral artery. *Middle cerebral artery* - The middle cerebral artery is a large artery that branches off the **internal carotid artery** and typically extends laterally and superiorly to supply a large part of the **cerebral hemispheres**. - It would appear more prominent and more laterally positioned, not forming a direct "communicating" link in the central Circle of Willis as shown. *Internal carotid artery* - The internal carotid artery ascends from the neck into the skull and bifurcates into the **anterior and middle cerebral arteries**. - While visible in the image, the arrow is pointing to a smaller anastomotic branch, not the main trunk of the internal carotid artery. *Anterior communicating artery* - The **anterior communicating artery** connects the two **anterior cerebral arteries** at the anterior aspect of the Circle of Willis. - This is a distinct location from that indicated by the arrow, which shows a vessel connecting anterior to posterior circulation, not linking the two anterior cerebral arteries.
Question 2: What is the name of the marked blood vessel in the Circle of Willis?
- A. Middle cerebral artery
- B. Posterior communicating artery (Correct Answer)
- C. Internal carotid artery
- D. Posterior cerebral artery
Explanation: ***Posterior communicating artery*** - The image displays the Circle of Willis, and the vessel marked with 'X' is connecting the **internal carotid artery** (which branches into the middle and anterior cerebral arteries) to the **posterior cerebral artery**. - This connecting artery is the **posterior communicating artery**, an essential component of the Circle of Willis, ensuring collateral blood flow to the brain. *Middle cerebral artery* - The **middle cerebral artery** branches off the internal carotid artery and typically extends laterally into the Sylvian fissure, supplying a large part of the lateral cerebral cortex. - The marked vessel is clearly connecting proximal arteries within the Circle of Willis, not extending into the cerebral cortex peripherally. *Internal carotid artery* - The **internal carotid artery** enters the skull and gives rise to several branches, including the middle cerebral artery and the posterior communicating artery. - While it's part of the supply to the Circle of Willis, the 'X' points specifically to the **communicating segment** connecting the anterior and posterior circulations, not the main trunk of the internal carotid. *Posterior cerebral artery* - The **posterior cerebral artery** is formed by the bifurcation of the basilar artery and supplies the occipital lobe and parts of the temporal lobe. - The marked vessel is connecting to the posterior cerebral artery, but it is not the posterior cerebral artery itself; rather, it is the vessel **communicating** with it from the anterior circulation.
Question 3: All of the following layers are pierced by the needle shown below except:
- A. Supraspinous ligament
- B. Inter-spinous ligament
- C. Ligamentum flavum
- D. Ligamentum denticulatum (Correct Answer)
Explanation: ***Ligamentum denticulatum*** - The **ligamentum denticulatum** is an internal structure of the spinal cord (specifically, pia mater extensions) and is not pierced during an LP, which targets the subarachnoid space. - It functions to suspend the spinal cord within the dura mater and is not in the pathway of the needle during a lumbar puncture. *Supraspinous ligament* - This ligament is the **first major ligament** encountered posterior to the spinous processes in the midline and must be pierced by the needle during a lumbar puncture. - It runs along the tips of the spinous processes. *Inter-spinous ligament* - Located between the spinous processes, this ligament is encountered **after the supraspinous ligament** and must be pierced during a lumbar puncture to reach deeper structures. - It connects adjacent spinous processes. *Ligamentum flavum* - This ligament is rich in elastic fibers and is pierced **before entering the epidural space** on the way to the subarachnoid space. - Its piercing is often felt as a distinct "pop" or "give" by the clinician performing the lumbar puncture.
Question 4: All investigations are useful in work up of this condition except:
- A. Urine for meconium particles
- B. Invertogram at 24 hours (Correct Answer)
- C. Ultrasound
- D. Lateral pelvic radiography
Explanation: ***Urine for meconium particles*** - **Urine for meconium particles** is actually a valuable and standard investigation in **anorectal malformations** to detect **rectourinary fistulas**. - The presence of meconium in urine indicates a **communication between the rectum and urinary tract**, which is crucial information for surgical planning and management. *Invertogram at 24 hours* - An **invertogram** is a plain X-ray taken with the infant inverted for 3-5 minutes, allowing gas in the rectum to rise to the highest point. - This helps determine the **level of rectal pouch termination** relative to the **pubococcygeal line**, which is essential for distinguishing between high and low anorectal malformations. *Ultrasound* - **Perineal ultrasound** can assess the **perineal body thickness**, presence of a **rectal pouch**, and help visualize **fistulous connections**. - It is particularly useful in **real-time assessment** of the anatomy and can identify associated **genitourinary anomalies** commonly seen with anorectal malformations. *Lateral pelvic radiography* - A **lateral pelvic radiograph** provides information about the **sacral anatomy** and helps assess the **level of anorectal malformation**. - It is crucial for identifying associated **sacral anomalies** (sacral dysgenesis, hemisacrum) which occur in up to 60% of patients with anorectal malformations and affect surgical outcomes.
Question 5: A 2-day-old neonate under phototherapy unit. For exchange transfusion serum bilirubin-albumin ratio should be: (Recent NEET Pattern 2016-17)
- A. $>3.5$ (Correct Answer)
- B. $<3.5$
- C. $>35$
- D. $<35$
Explanation: ***$>3.5$*** - A **serum bilirubin-albumin ratio greater than 3.5** is a common guideline indicating the need for exchange transfusion in neonates, especially those at high risk or with rapidly rising bilirubin levels. - This ratio helps assess the risk of **bilirubin-induced neurotoxicity (kernicterus)**, as unbound (free) bilirubin can cross the blood-brain barrier [1]. *$<3.5$* - A bilirubin-albumin ratio **less than 3.5** typically suggests a lower risk of neurotoxicity and may indicate that phototherapy is sufficient to manage hyperbilirubinemia [2]. - In such cases, the **binding capacity of albumin** for bilirubin is considered adequate to prevent significant free bilirubin accumulation [1]. *$>35$* - A serum bilirubin-albumin ratio of **greater than 35** would represent an extremely high and clinically improbable value. - Clinically, the bilirubin-albumin ratio is typically used with values in the single digits, making a value of 35 or higher incongruent with standard medical guidelines. *$<35$* - While technically true that $<35$ would include the correct threshold, it is not sufficiently specific to denote the critical value for exchange transfusion. - This range is too broad and does not pinpoint the specific bilirubin-albumin ratio that prompts intervention.
Question 6: What is correct about the composition of fluid in the area marked as $X$ ?
- A. Na = 150 mEq/L, K = 3 mEq/L, Chloride = 125 mEq/L
- B. Na = 3 mEq/L, K = 150 mEq/L, Chloride = 125 mEq/L (Correct Answer)
- C. Na = 50 mEq/L, K = 30 mEq/L, Chloride = 125 mEq/L
- D. Na = 150 mEq/L, K = 30 mEq/L, Chloride = 125 mEq/L
Explanation: ***Na = 3 mEq/L, K = 150 mEq/L, Chloride = 125 mEq/L*** - The area marked 'X' represents the **scala media** in the cochlear cross-section, which contains **endolymph**. - Endolymph has a unique ionic composition with **high potassium concentration** (150 mEq/L) and **low sodium concentration** (3 mEq/L), similar to intracellular fluid. *Na = 150 mEq/L, K = 3 mEq/L, Chloride = 125 mEq/L* - This composition represents **perilymph**, found in the **scala vestibuli** and **scala tympani**, not in the scala media. - Perilymph has high Na+ and low K+ concentrations, resembling **cerebrospinal fluid** and extracellular fluid. *Na = 150 mEq/L, K = 30 mEq/L, Chloride = 125 mEq/L* - The **potassium level of 30 mEq/L** is intermediate and doesn't match any physiological cochlear fluid composition. - This value is too high for perilymph (normally 3 mEq/L) and too low for endolymph (normally 150 mEq/L). *Na = 50 mEq/L, K = 30 mEq/L, Chloride = 125 mEq/L* - The **sodium concentration of 50 mEq/L** is abnormally low for any extracellular fluid compartment. - Neither the Na+ nor K+ values correspond to the known ionic gradients essential for **cochlear hair cell function**.
Question 7: All are correct about the part marked as $X$ and $Y$ except:
- A. $X$ is utricle and has anterior upward slope of 30 degrees (Correct Answer)
- B. $Y$ is ductus reuniens
- C. $Y$ connects utricle to cochlear duct
- D. $X$ is utricle and receives 5 openings of three semicircular canals
Explanation: This is an EXCEPT question - we need to identify the **incorrect** statement. ***$X$ is utricle and has anterior upward slope of 30 degrees*** ✓ **INCORRECT STATEMENT - This is the answer** - The **utricle's macula** is oriented **horizontally** when the head is in normal anatomical position, NOT at a 30-degree anterior upward slope - It is the **saccule's macula** that has an orientation closer to vertical (approximately 30° from vertical in some references) - The utricle detects **linear acceleration in the horizontal plane** - **This statement is FALSE, making it the correct answer to this EXCEPT question** *$X$ is utricle and receives 5 openings of three semicircular canals* ✓ **CORRECT STATEMENT** - This is anatomically **correct**. The utricle receives **five openings** from the three semicircular canals - The three semicircular canals (anterior, posterior, and lateral) have five openings because the **anterior and posterior canals share a common crus** - **This statement is TRUE, so it is not the answer** *$Y$ is ductus reuniens* ✓ **INCORRECT STATEMENT (but see note)** - $Y$ appears to point to the **saccule**, which is one of the **otolith organs** in the vestibule - The **ductus reuniens** is a small duct that connects the saccule to the cochlear duct, not the saccule itself - However, **without seeing the image**, if Y points to the ductus reuniens itself, this could be correct - Based on typical anatomy diagrams, Y most likely indicates the saccule, making this statement incorrect *$Y$ connects utricle to cochlear duct* ✓ **INCORRECT STATEMENT** - $Y$ is the **saccule**, not a connecting duct - The saccule connects to the cochlear duct via the **ductus reuniens** - The saccule does NOT directly connect the utricle to the cochlear duct - Anatomically, the utricle and saccule connect via the **utriculosaccular duct** **Key Point**: Since this is an EXCEPT question asking "All are correct EXCEPT", only **Option A** is the definitively FALSE statement about the anatomy. Options B and C are also incorrect statements, but Option A is the clearest incorrect statement based on standard anatomical orientation of the utricle's macula.
Question 8: All are true about the terminal area marked 'X' in this bacteria except:
- A. Volutin granules
- B. Strongly eosinophilic (Correct Answer)
- C. Function as storage reservoir for phosphate
- D. Also found in Yersinia pestis
Explanation: ***Strongly eosinophilic*** - The terminal areas marked 'X' represent **metachromatic granules** (also called volutin granules) which stain reddish-purple with methylene blue, a basic dye, indicating they are **basophilic**, not eosinophilic. - Eosinophilic structures stain well with acidic dyes like eosin, resulting in a pink or red color. *Volutin granules* - The terminal areas marked 'X' are characteristic **volutin granules**, also known as **metachromatic granules**, which are inclusions seen in certain bacteria. - These granules are prominent in *Corynebacterium diphtheriae*, which typically exhibits a **club-shaped** or **cuneiform** morphology. *Function as storage reservoir for phosphate* - Volutin granules primarily serve as a **storage reservoir for inorganic polyphosphate**, which is crucial for the bacterium's energy metabolism and various cellular processes. - This stored phosphate can be utilized when environmental phosphate levels are low. *Also found in Yersinia pestis* - **Bipolar staining**, which resembles prominent granules at the ends of the bacteria (similar to the appearance of volutin granules), is a characteristic feature of *Yersinia pestis*. - This gives *Yersinia pestis* a distinctive "safety pin" appearance on Wright-Giemsa or Wayson stain.
Question 9: Which of the following is correct about the image shown?
- A. A = Monotrichous, B = Lophotrichous, C = Amphitrichous, D = Peritrichous (Correct Answer)
- B. A = Lophotrichous, B = Monotrichous, C = Amphitrichous, D = Peritrichous
- C. A = Monotrichous, B = Lophotrichous, C = Peritrichous, D = Amphitrichous
- D. A = Peritrichous, B = Lophotrichous, C = Amphitrichous, D = Monotrichous
Explanation: ***A = Monotrichous, B = Lophotrichous, C = Amphitrichous, D = Peritrichous*** - Image **A** shows a bacterium with a **single flagellum at one pole**, which is the classic presentation of **Monotrichous** flagellation. - Image **B** depicts a bacterium with a **tuft of multiple flagella originating from one pole**, characteristic of **Lophotrichous** arrangement. - Image **C** shows a bacterium with **single flagella at both opposite poles**, consistent with **Amphitrichous** flagellation. - Image **D** demonstrates **flagella distributed uniformly over the entire bacterial cell surface**, which is the defining feature of **Peritrichous** flagellation. - This option correctly identifies all four flagellar arrangements as per standard microbiological classification. *A = Lophotrichous, B = Monotrichous, C = Amphitrichous, D = Peritrichous* - Incorrectly identifies image A as **Lophotrichous** (which requires multiple flagella at one pole), when it clearly shows only a single flagellum. - Also incorrectly labels image B as **Monotrichous** (single flagellum), when it displays a tuft of multiple flagella at one pole. *A = Monotrichous, B = Lophotrichous, C = Peritrichous, D = Amphitrichous* - Incorrectly identifies image C as **Peritrichous**, but the image shows flagella only at two opposite poles, not distributed all over the cell. - Misidentifies image D as **Amphitrichous** (flagella at two poles only), when it clearly shows flagella covering the entire bacterial surface. *A = Peritrichous, B = Lophotrichous, C = Amphitrichous, D = Monotrichous* - Incorrectly labels image A as **Peritrichous** (flagella all over), when it shows a single polar flagellum characteristic of Monotrichous arrangement. - Misidentifies image D as **Monotrichous** (single flagellum), when it demonstrates the peritrichous pattern with flagella distributed over the entire surface.
Question 10: Which of the following bacteria will have following appearance?
- A. Vibrio cholerae
- B. Alcaligenes faecalis (Correct Answer)
- C. Spirilla
- D. Salmonella typhi
Explanation: ***Alcaligenes faecalis*** - The image shown is a **rod-shaped bacterium** with a **tuft of flagella at each pole**, resulting in a **bipolar flagellation** pattern typical of *Alcaligenes faecalis*. - This arrangement of flagella (amphitrichous) is characteristic for motility in this specific bacterium. *Vibrio cholerae* - *Vibrio cholerae* is a **curved rod** (comma-shaped) and typically possesses a **single polar flagellum** (monotrichous), which is different from the structure shown. - Its unique shape and flagellar arrangement are key identifiers in microbiology. *Spirilla* - **Spirilla** are **spiral-shaped bacteria** with a rigid, wavy form, which is distinctly different from the rod shape depicted in the image. - They can have various flagellar arrangements, but their overall morphology is elongated and coiled, not straight. *Salmonella typhi* - *Salmonella typhi* is a **rod-shaped bacterium** but it is typically **peritrichous**, meaning it has flagella distributed all over its cell surface, not just at the poles. - The image clearly shows flagella only at the ends, ruling out *Salmonella typhi*.