NEET-PG 2017
353 Previous Year Questions with Answers & Explanations
General Medicine
4 questionsWhich of the following finding is shown in the chest leads?
Cannon A waves are seen in the JVP of a patient. ECG shows:
A patient develops missed beats after thrombolysis for MI. ECG shows:
A 12-year-old child with renal tubular acidosis type I is having muscle cramps and weakness. ECG shows all except:
NEET-PG 2017 - General Medicine NEET-PG Practice Questions and MCQs
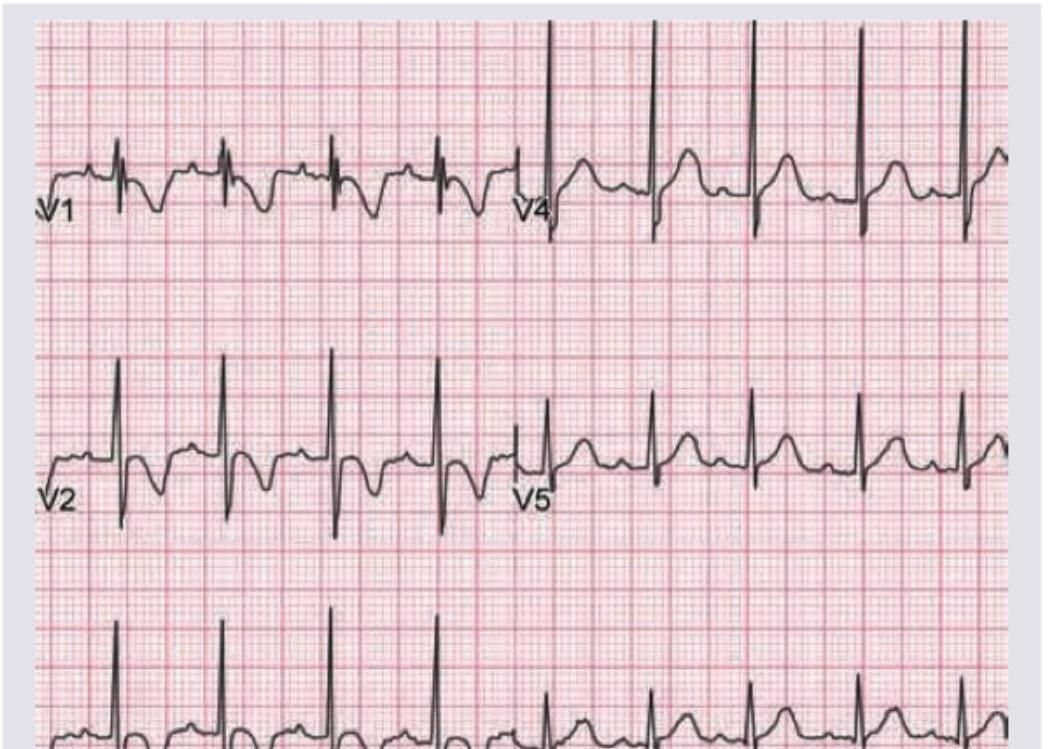
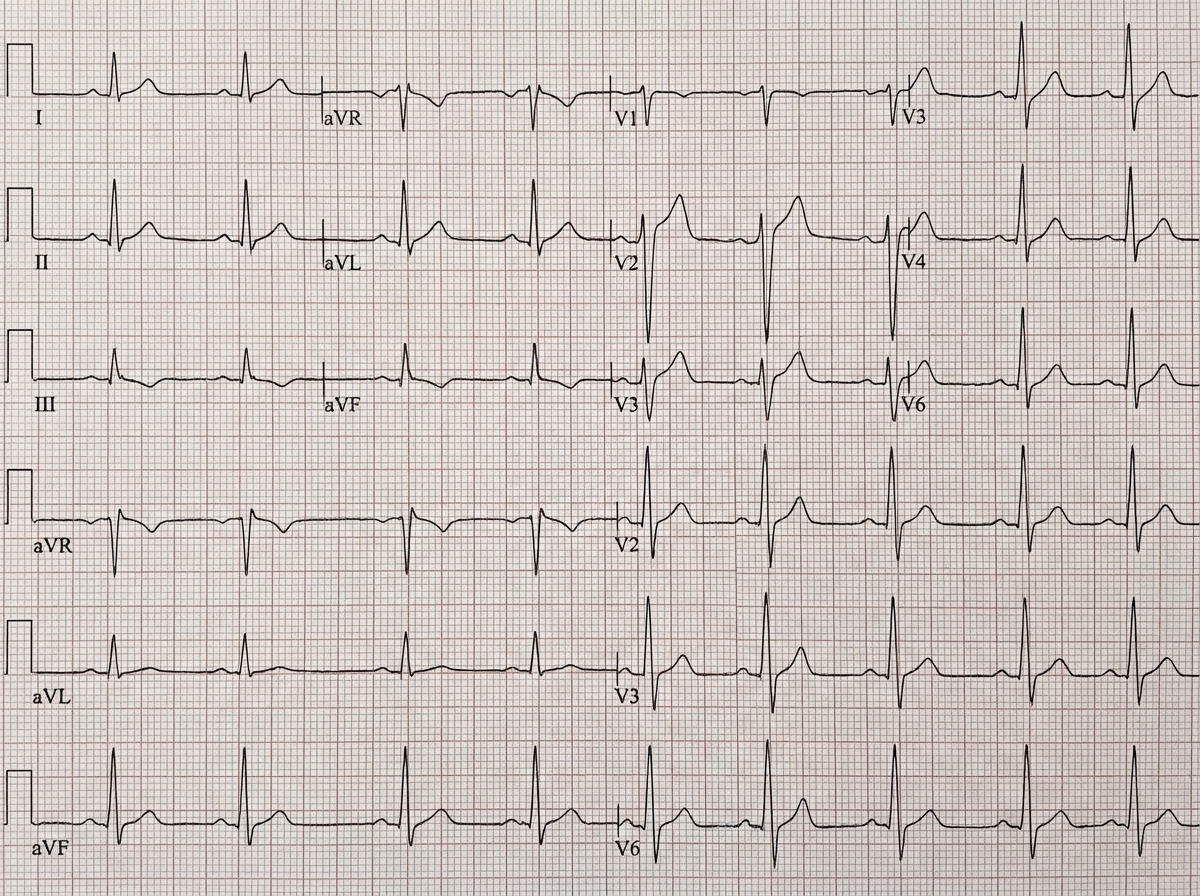
Question 1: Which of the following finding is shown in the chest leads?
- A. Myocardial ischemia
- B. Myocardial injury
- C. Digoxin (Correct Answer)
- D. Digoxin toxicity
Explanation: ***Digoxin*** - The ECG shows a characteristic **downward sloping ST segment depression** with a "sagging" or "scooped" appearance, often referred to as a **"Salvador Dali mustache"** appearance, which is typical of digoxin effect on the ECG. - This pattern is due to the drug's effect on **myocardial repolarization**, specifically shortening the QT interval and inducing these ST changes, even in the absence of toxicity. *Myocardial ischemia* - Myocardial ischemia typically manifests as **ST segment depression** that is **horizontal** or **downsloping** but usually not with the characteristic "scooped" appearance seen with digoxin. - T-wave inversions may also be present, which are not the primary finding here. *Myocardial injury* - Acute myocardial injury is characterized by **ST segment elevation** (in acute myocardial infarction) or **significant ST depression with T-wave inversions** (in NSTEMI) which differs from the morphology seen in this ECG. - The morphology of the ST segment in myocardial injury is usually more abrupt and not "scooped" like a digoxin effect. *Digoxin toxicity* - While this ECG shows a digoxin effect, **digoxin toxicity** usually presents with **arrhythmias** (e.g., ventricular premature beats, bradycardia, AV blocks) in addition to altered ST-T wave morphology. - The ECG alone, showing only repolarization changes characteristic of digoxin, does not confirm toxicity without clinical correlation or evidence of arrhythmias.
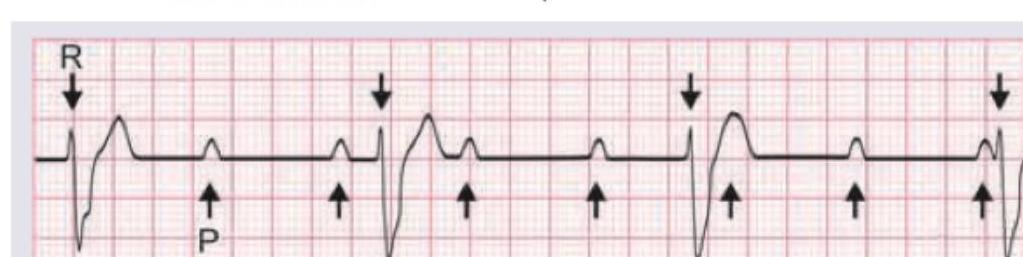
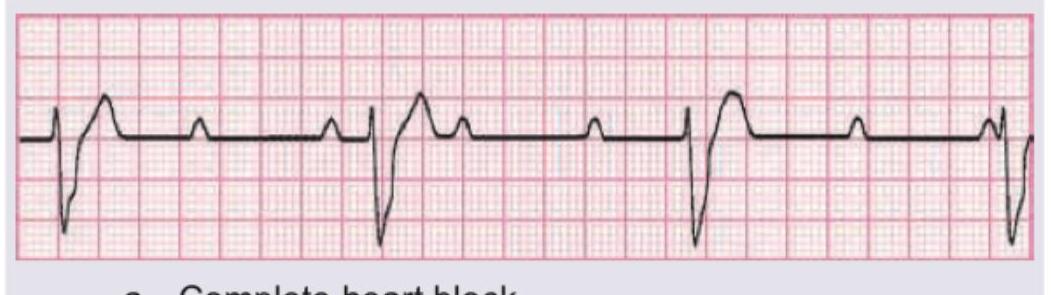
Question 2: Cannon A waves are seen in the JVP of a patient. ECG shows:
- A. First degree heart block
- B. Second degree heart block
- C. Third degree heart block (Correct Answer)
- D. Mobitz II heart block
Explanation: ***Third degree heart block*** - **Cannon A waves** in the JVP occur when the right atrium contracts against a closed tricuspid valve, which happens when atrial and ventricular contractions are **dissociated** as seen in **complete heart block**. - In the provided ECG, there is complete dissociation between P waves (atrial activity) and QRS complexes (ventricular activity), with P waves occurring regularly but independently of the QRS complexes, which signifies a **third-degree (complete) heart block**. *First degree heart block* - Characterized by a **prolonged PR interval** (>0.20 seconds) where every P wave is followed by a QRS complex. - There is no dissociation of P waves and QRS complexes, and therefore no cannon A waves due to atrial contraction against a closed tricuspid valve. *Second degree heart block* - Involves some P waves not being followed by a QRS complex, indicating **intermittent conduction failure**. - There can be Wenckebach (Mobitz I) or Mobitz II, both of which involve some degree of P-wave-QRS coupling, usually not leading to constant or prominent cannon A waves. *Mobitz II heart block* - Defined by intermittently **dropped QRS complexes** without progressive PR lengthening, often with a constant PR interval before the drop. - While some dropped beats occur, there is still a clear relationship between the P waves and the conducted QRS complexes, which differs from the continuous and complete AV dissociation seen with cannon A waves in third-degree block.
Question 3: A patient develops missed beats after thrombolysis for MI. ECG shows:
- A. Mobitz I heart block (Correct Answer)
- B. Mobitz II heart block
- C. Complete heart block
- D. Sick sinus syndrome
Explanation: ***Mobitz I heart block*** - The ECG shows a **progressive lengthening of the PR interval** before a QRS complex is dropped (missed beat), which is characteristic of Mobitz type I (Wenckebach) heart block. - This type of block is often **benign** and located in the AV node, frequently resolving spontaneously, especially after thrombolysis for an inferior MI. *Mobitz II heart block* - Characterized by **sudden, unexpected dropped QRS complexes** without prior PR interval lengthening. - Mobitz II usually indicates a block below the AV node (infranodal) and is considered more serious, often requiring a pacemaker. *Complete heart block* - In complete (third-degree) heart block, there is **no conduction between the atria and ventricles**, meaning P waves and QRS complexes are completely dissociated. - The ventricular rhythm is typically slow and independent of the atrial rhythm, which is not seen here as some P waves conduct. *Sick sinus syndrome* - Sick sinus syndrome is a **dysfunction of the SA node**, leading to various arrhythmias such as sinus bradycardia, sinus arrest, or sinoatrial block. - While it can cause missed beats, the ECG pattern here specifically points to a problem with AV conduction (PR interval changes and dropped QRS), not primary sinus node dysfunction.
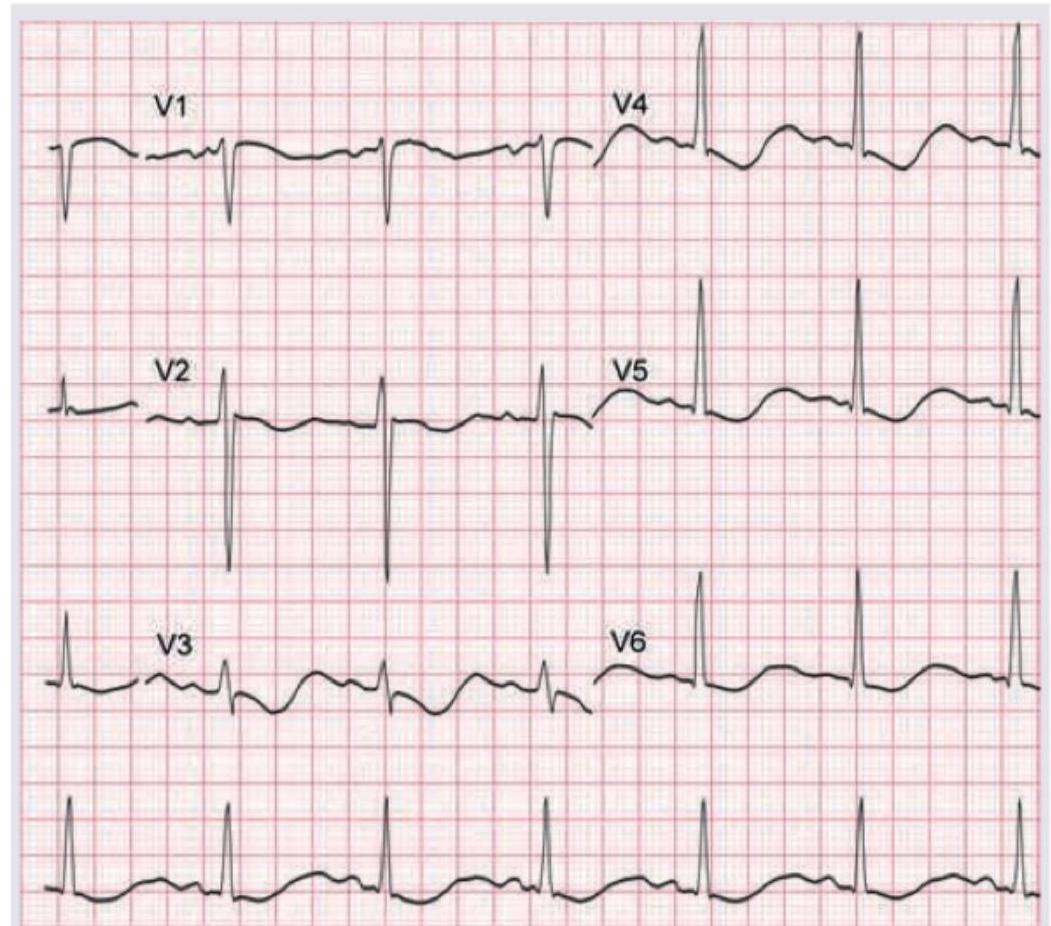
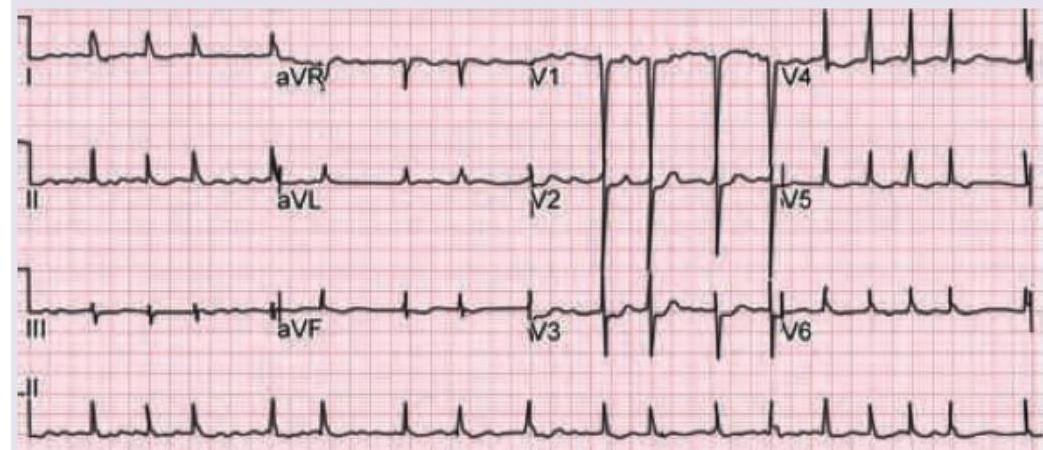
Question 4: A 12-year-old child with renal tubular acidosis type I is having muscle cramps and weakness. ECG shows all except:
- A. T wave inversion with U waves
- B. ST depression
- C. Heart rate of 75 beats per minute
- D. Absent P waves (Correct Answer)
Explanation: ***Absent P waves*** - **Hypokalemia (low potassium)**, common in renal tubular acidosis type I, does not typically cause absent P waves. Absent P waves are characteristic of certain **atrial arrhythmias** or severe **hyperkalemia** with sine wave formation. - The image provided clearly shows visible P waves before each QRS complex, indicating **sinus rhythm** and normal atrial depolarization. *T wave inversion with U waves* - **Hypokalemia** can cause characteristic ECG changes including **T wave flattening**, **T wave inversion**, and prominent **U waves**, especially in leads V2-V4. - The provided ECG shows evidence of T wave flattening or inversion and visible U waves, which are consistent with hypokalemia. *ST depression* - **ST depression** can occur in cases of significant **hypokalemia**, particularly when potassium levels are very low. - The ECG shows some subtle **ST segment depression**, especially in leads like V3, which is a recognized finding in hypokalemia. *Heart rate of 75 beats per minute* - To calculate the heart rate, count the number of large squares between two R waves (e.g., in V5, there are approximately 4 large squares). The heart rate is 300 / number of large squares = 300 / 4 = **75 bpm**. - A heart rate of 75 bpm is a **normal sinus rhythm** and is not inconsistent with hypokalemia.
Internal Medicine
3 questionsECG of a patient had ST segment elevation in V1-V6, lead I and AVL. Which of the following branches is involved?
A 35-year-old lady has been diagnosed with anxiety neurosis by her psychiatrist. She came to you for second opinion. Comment on the diagnosis based on ECG.
A 68-year-old postoperative patient who has undergone thyroidectomy presents with muscle cramps. ECG shows?
NEET-PG 2017 - Internal Medicine NEET-PG Practice Questions and MCQs
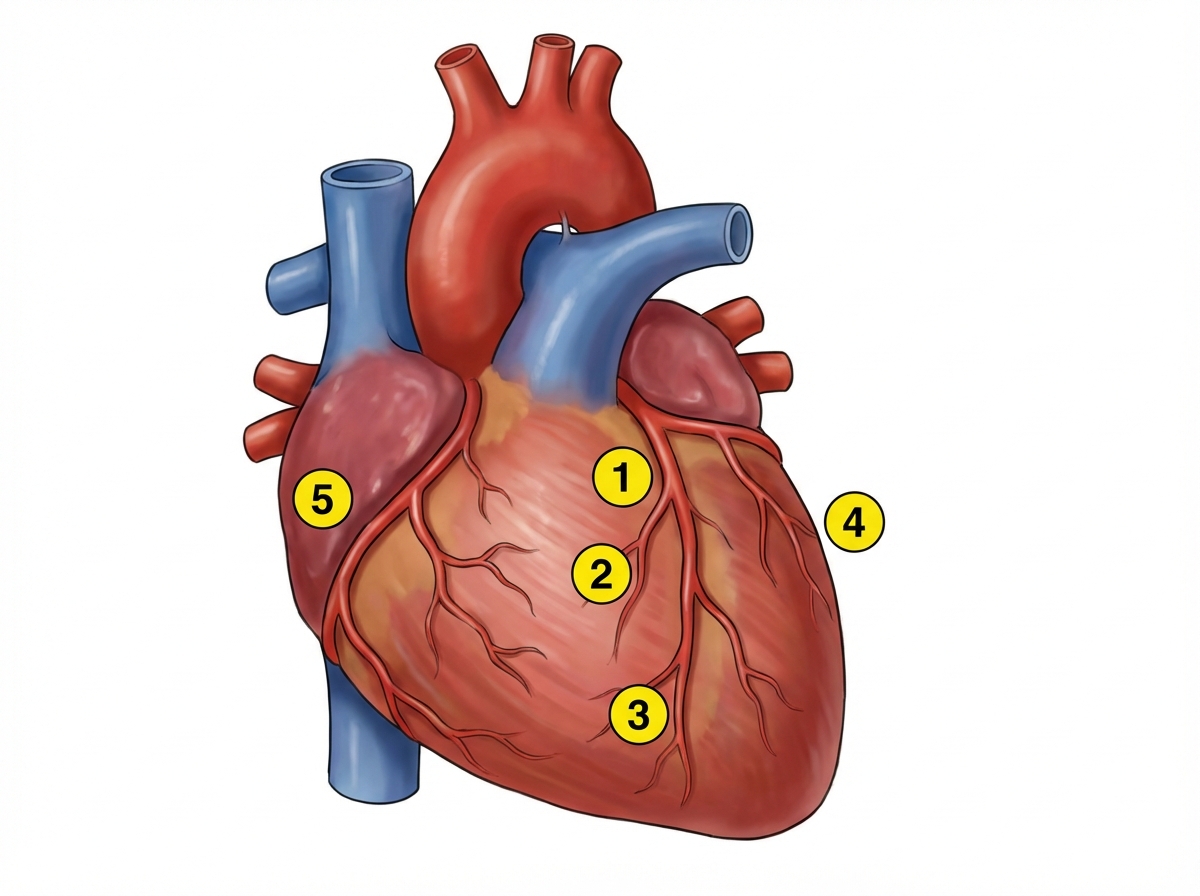
Question 1: ECG of a patient had ST segment elevation in V1-V6, lead I and AVL. Which of the following branches is involved?
- A. 1 (Correct Answer)
- B. 2
- C. 3
- D. 4
- E. 5
Explanation: ***1*** - The ECG findings of **ST segment elevation in V1-V6, lead I and aVL** indicate an **extensive anterior myocardial infarction**. This territory is supplied by the **left main coronary artery (LMCA)** and its major branch, the **left anterior descending (LAD) artery** (numbered as 1 in the image). - The image clearly labels **1 as the left anterior descending (LAD) artery**, which is responsible for perfusing the anterior wall, septum, and apex of the left ventricle. *2* - **2 points to a diagonal branch** stemming from the LAD artery. While occlusion of a diagonal branch can cause ST elevation, it would typically be more localized (e.g., in aVL and some precordial leads) and not as extensive as V1-V6. - A diagonal branch occlusion would not account for the **extensive anterior infarction** indicated by widespread precordial and high lateral lead ST elevation. *3* - **3 points to a more distal portion of the LAD artery** or one of its smaller distal branches. Occlusion here would cause an **apical or antero-septal infarction**, which is usually less extensive than an occlusion higher up. - The widespread ST elevation across V1-V6, I, and aVL suggests a more **proximal occlusion** affecting a larger myocardial territory, rather than just the distal LAD. *4* - **4 points to a marginal branch of the left circumflex artery (LCx)**. The LCx artery supplies the lateral wall of the left ventricle. - Occlusion of a marginal branch would typically result in **ST elevation in leads I, aVL, V5, and V6**, but would not cause ST elevation in the septal and anterior leads (V1-V4), which are indicative of LAD involvement. *5* - **5 points to the right coronary artery (RCA)** or its branches. The RCA supplies the inferior wall of the left ventricle, the right ventricle, and often the posterior wall. - Occlusion of the RCA would cause **ST elevation in leads II, III, and aVF** (inferior MI), not the anterior and lateral leads (V1-V6, I, aVL) seen in this case.
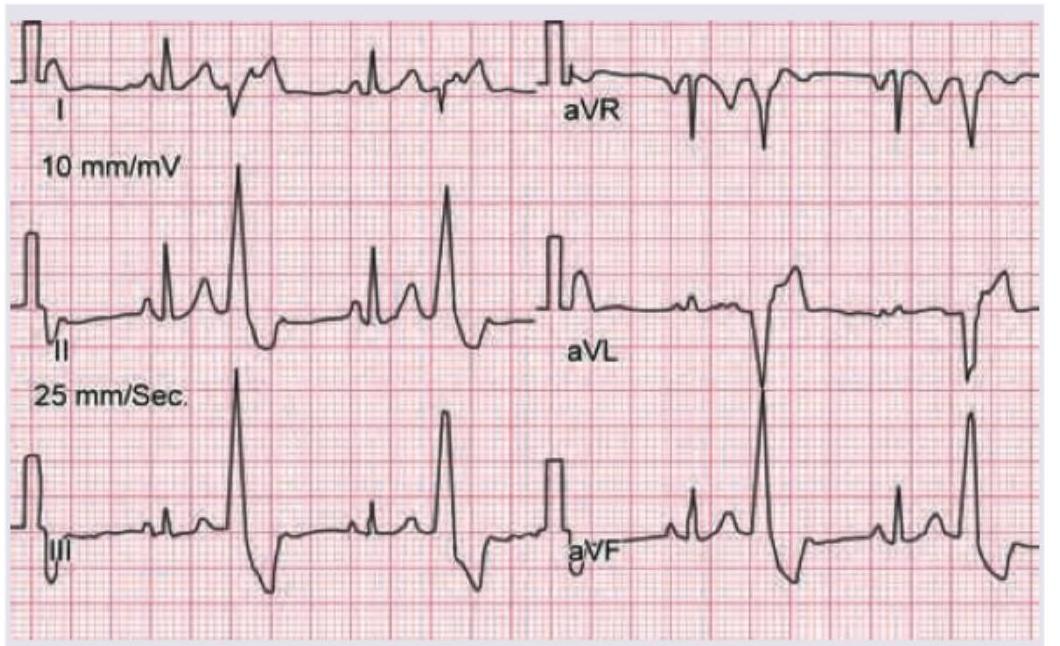
Question 2: A 35-year-old lady has been diagnosed with anxiety neurosis by her psychiatrist. She came to you for second opinion. Comment on the diagnosis based on ECG.
- A. Sinus tachycardia
- B. WPW syndrome (Correct Answer)
- C. Multifocal atrial tachycardia
- D. Atrial fibrillation
- E. Supraventricular tachycardia
Explanation: ***WPW syndrome*** - The ECG clearly shows a **short PR interval** and a **delta wave** (slurring of the initial part of the QRS complex), which are classic findings for **Wolff-Parkinson-White (WPW) syndrome**. - While anxiety neurosis can cause sinus tachycardia, the presence of a **pre-excitation pattern** on ECG indicates an underlying cardiac electrical abnormality that requires further evaluation and management, irrespective of the anxiety diagnosis. *Sinus tachycardia* - Sinus tachycardia would show a normal P wave before every QRS complex, a normal PR interval, and a heart rate >100 bpm. This ECG shows a **short PR interval** and a **delta wave**, which are not consistent with pure sinus tachycardia. - While anxiety can cause sinus tachycardia, the ECG findings here point to an **anatomical accessory pathway** rather than just a physiological response. *Supraventricular tachycardia* - While WPW syndrome can lead to **atrioventricular reentrant tachycardia (AVRT)**, a type of SVT, the ECG shown demonstrates the **baseline pre-excitation pattern** with delta waves, not an active tachyarrhythmia. - Classic SVT (such as AVNRT) during an episode would show a **narrow QRS complex** tachycardia with a regular rhythm and no delta waves, whereas this ECG shows the **characteristic delta wave** of WPW syndrome at baseline. *Multifocal atrial tachycardia* - Characterized by at least **three different P wave morphologies** and an irregular rhythm, which are not seen in this ECG. - The rhythm shown is regular, and the P wave morphology (or lack thereof before the delta wave) is consistent, ruling out multifocal atrial tachycardia. *Atrial fibrillation* - Atrial fibrillation would present with an **irregularly irregular rhythm**, absence of distinct P waves, and F waves (fibrillatory waves), none of which are evident in this ECG. - The ECG shows a regular rhythm with discernible complexes, inconsistent with the chaotic electrical activity of atrial fibrillation.
Question 3: A 68-year-old postoperative patient who has undergone thyroidectomy presents with muscle cramps. ECG shows?
- A. Prolonged QT interval (Correct Answer)
- B. Short QT interval
- C. ST elevation
- D. ST depression
Explanation: ***Prolonged QT interval*** - A patient who has undergone thyroidectomy and presents with muscle cramps likely has **hypocalcemia** due to inadvertent parathyroid gland removal. - Hypocalcemia is well-known to cause a **prolonged QT interval** on EKG, increasing the risk of arrhythmias. *Short QT interval* - A short QT interval is typically associated with **hypercalcemia** or genetic disorders. - This patient's presentation of muscle cramps is inconsistent with hypercalcemia. *ST elevation* - ST elevation is a hallmark of **acute myocardial infarction** or **pericarditis**. - This finding is unrelated to hypocalcemia or the patient's immediate postoperative and symptoms. *ST depression* - ST depression often indicates **myocardial ischemia** or **digoxin effect**. - It is not a characteristic ECG change associated with hypocalcemia or muscle cramps.
Pediatrics
2 questionsThe given ECG of a neonate born to a mother with SLE shows?
A 10-year-old child with Valvular heart disease on heart failure treatment, has the following ECG tracing. What is the diagnosis?
NEET-PG 2017 - Pediatrics NEET-PG Practice Questions and MCQs
Question 1: The given ECG of a neonate born to a mother with SLE shows?
- A. Complete heart block (Correct Answer)
- B. Mobitz I heart block
- C. Mobitz II heart block
- D. Sick sinus syndrome
Explanation: ***Complete heart block*** - The ECG demonstrates **complete dissociation** between the P waves (atrial activity) and the QRS complexes (ventricular activity). The atrial rate is faster than the ventricular rate, and there is no consistent relationship between P waves and QRS complexes. - In a neonate of a mother with SLE, **congenital complete heart block** is a well-known complication due to transplacental transfer of maternal antibodies (anti-Ro/SSA and anti-La/SSB) that damage the atrioventricular (AV) node. *Mobitz I heart block* - This type of heart block (also known as **Wenckebach phenomenon**) is characterized by a **progressive prolongation of the PR interval** until a P wave is eventually not conducted, leading to a dropped QRS complex. - The ECG provided does not show a gradual lengthening of the PR interval; rather, it shows a complete lack of conduction between atria and ventricles. *Mobitz II heart block* - In Mobitz II block, there is a **fixed PR interval** for conducted beats, but some P waves are **intermittently blocked** without prior PR prolongation. - The ECG in the question shows no consistent PR interval whatsoever, as P waves and QRS complexes are completely dissociated. *Sick sinus syndrome* - This condition involves a malfunction of the **sinoatrial node**, leading to a variety of rhythm disturbances such as sinus bradycardia, sinus arrest, or *tachycardia-bradycardia syndrome*. - While it can cause bradycardia, it does not typically present with the **P-QRS dissociation** characteristic of advanced AV block seen in the ECG.
Question 2: A 10-year-old child with Valvular heart disease on heart failure treatment, has the following ECG tracing. What is the diagnosis?
- A. Tall tented T-wave
- B. Ventricular bigeminy
- C. Non paroxysmal atrial tachycardia with irregular AV block
- D. Non paroxysmal atrial tachycardia with regular AV block (Correct Answer)
Explanation: ***Non paroxysmal atrial tachycardia with regular AV block*** - The ECG shows a sustained atrial tachycardia with a **consistent P-P interval**, indicating a non-paroxysmal origin. - There is a **fixed ratio between P waves and QRS complexes** (e.g., 2:1 or 3:1), demonstrating a regular AV block, likely due to increased vagal tone or AV nodal dysfunction, often seen in cases of **digoxin toxicity** (given the patient is on heart failure treatment for valvular heart disease). *Tall tented T-wave* - **Tall, tented T-waves** are characteristic of **hyperkalemia**, but the ECG tracing does not exhibit this morphology. - While hyperkalemia can cause rhythm disturbances, the predominant feature here is a regular atrial tachycardia with AV block, not T-wave changes typical of electrolyte imbalance. *Ventricular bigeminy* - **Ventricular bigeminy** would manifest as alternating normal QRS complexes with premature ventricular contractions (PVCs). - The ECG shows a narrow complex tachycardia with visible P waves, which are not characteristic of PVCs or ventricular bigeminy. *Non paroxysmal atrial tachycardia with irregular AV block* - Although there is non-paroxysmal atrial tachycardia, the **AV block is regular** (e.g., a consistent 2:1 or 3:1 conduction ratio), not irregular. - An irregular AV block would suggest variability in AV nodal conduction, such as in AV Wenckebach or Mobitz type II with variable conduction, which is not what is seen in this tracing.
Pharmacology
1 questionsA 50-year-old woman with rheumatic heart disease is on medication for heart disease. She feels unwell for most part of the day. Which of the following medicine is responsible for the ECG changes shown below? (Recent NEET Pattern 2016-17)
NEET-PG 2017 - Pharmacology NEET-PG Practice Questions and MCQs
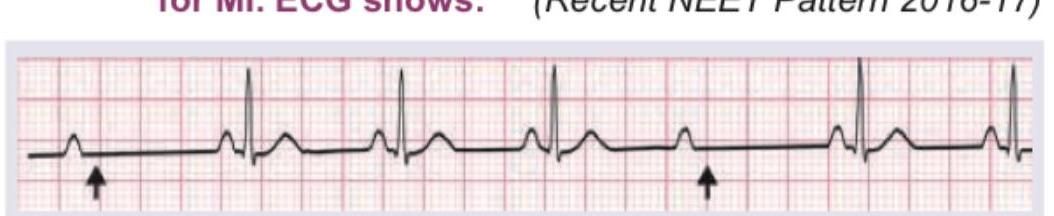
Question 1: A 50-year-old woman with rheumatic heart disease is on medication for heart disease. She feels unwell for most part of the day. Which of the following medicine is responsible for the ECG changes shown below? (Recent NEET Pattern 2016-17)
- A. ACE inhibitor
- B. Diuretics
- C. Ivabradine
- D. Digoxin (Correct Answer)
Explanation: ***Digoxin*** - The ECG shows changes characteristic of **digoxin toxicity**, specifically **downsloping ST depressions (scooping)** and **flattened or inverted T waves**, particularly in leads with dominant R waves. - The patient's symptoms of feeling "unwell for most part of the day" are consistent with **digoxin toxicity**, which can include nausea, fatigue, and cardiac arrhythmias. *ACE inhibitor* - ACE inhibitors primarily affect the **renin-angiotensin-aldosterone system** and do not typically cause these specific ECG changes. - Common side effects include cough and **hyperkalemia**, not the "scooped" ST segments seen here. *Diuretics* - Diuretics can cause **electrolyte imbalances**, such as hypokalemia, which might manifest as **flattened T waves** or **prominent U waves** on ECG, but not the characteristic "scooped" ST depression. - The symptoms of malaise are non-specific and while possible with electrolyte disturbances, the specific ECG pattern points away from diuretics as the primary cause. *Ivabradine* - Ivabradine is a **selective If channel inhibitor** that primarily reduces heart rate, without affecting myocardial contractility or repolarization significantly. - It does not cause the **ST segment changes** characteristic of digoxin effect or toxicity.
About NEET-PG 2017 Questions
This page contains 353 questions from the NEET-PG 2017 paper, organised across 22 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the NEET-PG exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your NEET-PG goals.