INI-CET 2023 — Pathology
14 Previous Year Questions with Answers & Explanations
Which of the following is an Anti-apoptotic gene?
Which of the following are characteristic laboratory findings in Iron Deficiency Anemia (IDA)? 1. Low serum ferritin 2. Low transferrin saturation 3. Low serum iron 4. Increased TIBC
Order of drawing blood in vacutainers should be in the following sequence to prevent contamination:
Which of the following cells is shown in the given image?
Match the following? a. Trisomy 13 1. Huntington disease b. Trisomy 18 2. Patau syndrome c. Trinucleotide repeat sequence 3. Sickle cell disease d. Hb point mutation of glutamate to valine 4. Edward syndrome
What is the correct statement about thymoma?
Which of the following conditions is associated with perineural invasion?
What is the interpretation of the given pedigree chart?
Identify the correct statement regarding Amyloidosis?
Match the following columns A. Caplan syndrome B. Mesothelioma C. Silicosis D. Asbestosis 1. Pleural effusion without shift 2. Crazy Paving 3. Lower lobe involved 4. Described in coal workers
INI-CET 2023 - Pathology INI-CET Practice Questions and MCQs
Question 1: Which of the following is an Anti-apoptotic gene?
- A. BAK
- B. BIN
- C. NOX-Q
- D. MCL-1 (Correct Answer)
Explanation: ***MCL-1*** - **MCL-1 (myeloid cell leukemia sequence 1)** is a pro-survival protein belonging to the **Bcl-2 family**, which inhibits apoptosis by binding to and sequestering pro-apoptotic proteins [1]. - Its overexpression is frequently observed in various cancers, contributing to **chemoresistance** and tumor survival [2]. *BAK* - **BAK (Bcl-2 antagonist killer 1)** is a **pro-apoptotic protein** that belongs to the Bcl-2 family. - Upon activation, BAK undergoes **oligomerization** on the mitochondrial outer membrane, leading to its permeabilization and the release of pro-apoptotic factors into the cytoplasm. *BIN* - **BIN1 (Bridging Integrator 1)** is a **tumor suppressor gene** that can promote apoptosis in certain contexts, particularly when associated with DNA damage or cellular stress. - It is not primarily known as an anti-apoptotic gene but rather as a protein involved in **membrane dynamics** and cellular signaling, with roles in endocytosis and cytoskeletal regulation. *NOX-Q* - **NOX-Q** is not a commonly recognized or established gene in the context of apoptosis regulation. - The **NOX (NADPH oxidase) family** of enzymes is primarily involved in the production of **reactive oxygen species (ROS)**, which can either induce or inhibit apoptosis depending on the cellular context and concentration. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, p. 310. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, pp. 310-311.
Question 2: Which of the following are characteristic laboratory findings in Iron Deficiency Anemia (IDA)? 1. Low serum ferritin 2. Low transferrin saturation 3. Low serum iron 4. Increased TIBC
- A. 3 and 4 only
- B. 1, 3, and 4 only
- C. 1 and 2 only
- D. All of the above (Correct Answer)
Explanation: ***All of the above (1, 2, 3, and 4)*** - **All listed parameters are characteristic findings in Iron Deficiency Anemia (IDA):** - **Low serum ferritin** - Indicates depleted iron stores; most specific early marker [1] - **Low serum iron** - Reflects reduced circulating iron availability [1] - **Low transferrin saturation** - Shows decreased percentage of iron-bound transferrin molecules (typically <15%) [1] - **Increased TIBC** - Compensatory increase in total iron-binding capacity as the liver produces more transferrin to capture available iron [1] *Why not just 1, 2, and 3?* - Increased TIBC is also a hallmark finding in IDA, distinguishing it from anemia of chronic disease (where TIBC is typically low) [1] *Why not just 3 and 4?* - Serum ferritin and transferrin saturation are equally important diagnostic parameters [1] *Why not just 1, 3, and 4?* - Low transferrin saturation is a key diagnostic criterion for IDA [1] **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Red Blood Cell and Bleeding Disorders, pp. 657-660.
Question 3: Order of drawing blood in vacutainers should be in the following sequence to prevent contamination:
- A. Plain → Blood culture → Citrate → EDTA → Fluoride
- B. Citrate → Blood culture → Plain → EDTA → Fluoride
- C. Blood culture → Plain → EDTA → Citrate → Fluoride
- D. Blood culture → Citrate → Plain → EDTA → Fluoride (Correct Answer)
Explanation: ***Blood culture → Citrate → Plain → EDTA → Fluoride*** - This sequence is the recommended order of draw to prevent **cross-contamination** between different additives, which could interfere with laboratory test results. - Starting with **blood cultures** minimizes contamination risk for microbiological analysis [1], followed by tubes containing anticoagulants like **citrate** (for coagulation studies), then **plain** tubes (for serum), followed by **EDTA** (for hematology), and finally **fluoride** (for glucose). - This order prevents carryover of additives that could affect subsequent test results. *Plain → Blood culture → Citrate → EDTA → Fluoride* - Drawing a **plain tube** first is incorrect as it might introduce skin flora into the blood culture bottle if performed later. - **Blood culture** should always be drawn first to ensure sterility and prevent contamination from other tube additives [1]. *Citrate → Blood culture → Plain → EDTA → Fluoride* - Drawing the **citrate tube** before blood culture is incorrect due to the risk of introducing citrate anticoagulant into the blood culture, which could inhibit bacterial growth. - The **blood culture** bottle requires the highest priority for sterility [1]. *Blood culture → Plain → EDTA → Citrate → Fluoride* - Placing the **plain tube** before **citrate tube** is incorrect according to CLSI guidelines. - Drawing the **EDTA tube** before the **citrate tube** can lead to contamination of the citrate sample with EDTA, potentially affecting coagulation tests by chelating calcium. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Cardiovascular Disease, pp. 296-297.
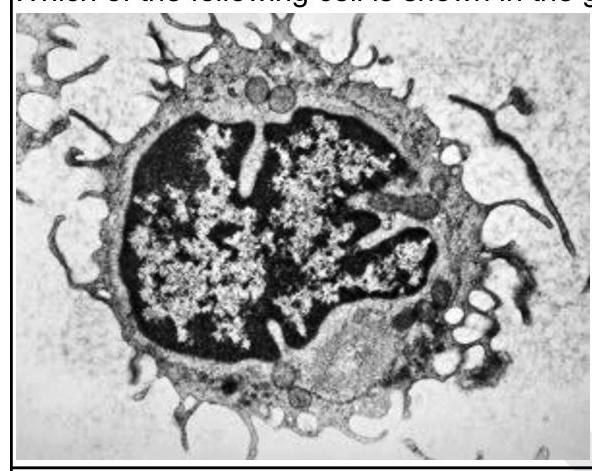
Question 4: Which of the following cells is shown in the given image?
- A. Hairy cell (Correct Answer)
- B. Sickle cell
- C. Gaucher cell
- D. Target cell
Explanation: ***Hairy cell*** - The image displays prominent **cytoplasmic projections** or "hairs" on the cell surface, which are characteristic features of **hairy cells** (lymphocytes seen in hairy cell leukemia) [1]. - These cells typically have an irregularly shaped nucleus and cytoplasm rich in ribosomes, as suggested by the granular appearance [1]. *Sickle cell* - **Sickle cells** are **red blood cells** that have a characteristic crescent or sickle shape due to abnormal hemoglobin polymerization. - The cell in the image is a **white blood cell** with a large nucleus and cytoplasmic extensions, clearly not a red blood cell. *Gaucher cell* - **Gaucher cells** are **macrophages** that accumulate glucocerebroside, giving them a characteristic **"crinkled paper"** or **"chicken scratch"** cytoplasm. - While they are large cells, they lack the distinct, fine, hair-like projections seen in the provided image. *Target cell* - **Target cells** are **red blood cells** with a central bullseye appearance due to an abnormal distribution of hemoglobin, often seen in thalassemia or liver disease. - The presented image is not a red blood cell and does not demonstrate the morphology of a target cell. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, p. 612.
Question 5: Match the following? a. Trisomy 13 1. Huntington disease b. Trisomy 18 2. Patau syndrome c. Trinucleotide repeat sequence 3. Sickle cell disease d. Hb point mutation of glutamate to valine 4. Edward syndrome
- A. b1-a3-d2-c4
- B. a2-b4-c1-d3 (Correct Answer)
- C. a2-b1-c4-d3
- D. a4-b1-c3-d2
Explanation: ***a2-b4-c1-d3*** - **Trisomy 13 (Patau syndrome)**: Chromosomal disorder with severe CNS malformations, holoprosencephaly, cleft lip/palate, and polydactyly [3] - **Trisomy 18 (Edward syndrome)**: Chromosomal disorder with clenched fists, rocker-bottom feet, and cardiac defects [3] - **Trinucleotide repeat sequence (Huntington disease)**: CAG repeat expansion in HTT gene causing progressive neurodegeneration with chorea and cognitive decline [2] - **Hb point mutation glutamate to valine (Sickle cell disease)**: Point mutation in β-globin gene (Glu6Val) causing hemoglobin polymerization and sickling [1] *b1-a3-d2-c4* - Incorrectly matches Trisomy 13 with sickle cell disease (point mutation, not trisomy) - Incorrectly matches Trisomy 18 with Huntington disease (trinucleotide repeat, not trisomy) - Incorrectly matches trinucleotide repeats with Edward syndrome (trisomy 18, not repeat expansion) *a2-b1-c4-d3* - Incorrectly matches Trisomy 18 with Huntington disease (trinucleotide repeat disorder, not chromosomal) - Incorrectly matches trinucleotide repeats with Edward syndrome (trisomy, not repeat expansion) *a4-b1-c3-d2* - Incorrectly matches Trisomy 13 with Edward syndrome (Trisomy 13 is Patau, not Edward) - Incorrectly matches Trisomy 18 with Huntington disease (trinucleotide repeat, not trisomy) - Incorrectly matches trinucleotide repeats with sickle cell disease (point mutation, not repeat expansion) **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Cellular Responses to Stress and Toxic Insults: Adaptation, Injury, and Death, pp. 50-51. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, p. 177. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 92-93.
Question 6: What is the correct statement about thymoma?
- A. Chest X-ray is the investigation of choice for the diagnosis of thymoma.
- B. Thymoma is primarily located in the posterior mediastinum.
- C. Thymoma is the most common neoplasia of the thymus. (Correct Answer)
- D. Thymoma is usually asymptomatic and only occasionally causes symptoms.
Explanation: ***Thymoma is the most common neoplasia of the thymus.*** [1] - **Thymoma** is the most common primary tumor of the thymus, accounting for approximately **40-50% of anterior mediastinal masses** in adults. - It is a slow-growing tumor originating from the **epithelial cells** of the thymus [1]. *Chest X-ray is the investigation of choice for the diagnosis of thymoma.* - While a **chest X-ray** may show a widened mediastinum or an anterior mediastinal mass, it is not the investigation of choice for definitive diagnosis or staging [2]. - **CT scan** of the chest with contrast is the preferred imaging modality for evaluating thymomas, providing better anatomical detail and assessing invasiveness [2]. *Thymoma is typically asymptomatic and rarely causes any symptoms.* - Approximately **30-50% of patients with thymoma are asymptomatic** at diagnosis, with the tumor discovered incidentally on imaging [2]. - However, the remaining **50-70% of patients present with symptoms** related to **mass effect** (e.g., chest pain, dyspnea, cough) or **paraneoplastic syndromes** like myasthenia gravis, pure red cell aplasia, or hypogammaglobulinemia [2]. - Therefore, it is incorrect to say thymoma "rarely" causes symptoms. *Thymoma is primarily located in the posterior mediastinum.* - **Thymoma** is characteristically located in the **anterior mediastinum**, which is the most common site for thymic tissue. - Tumors primarily found in the posterior mediastinum are more commonly **neurogenic tumors**. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 571-574. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 572-574.
Question 7: Which of the following conditions is associated with perineural invasion?
- A. Mucoepidermoid tumor
- B. Pancreatic cancer
- C. Pleomorphic adenoma
- D. Adenoid cystic carcinoma (Correct Answer)
Explanation: ***Adenoid cystic carcinoma*** - **Adenoid cystic carcinoma** is the **most notoriously characterized** by its strong propensity for **perineural invasion**, which contributes to its high recurrence rate and poor prognosis [1]. - This invasion allows the tumor cells to spread along nerve sheaths, extending beyond the visible tumor margins, often for considerable distances. - It is the **classic example** of perineural invasion among salivary gland tumors [1]. *Mucoepidermoid tumor* - While mucoepidermoid tumors can be locally aggressive, **perineural invasion** is not a characteristic feature that defines this tumor type. - They are more commonly associated with cystic degeneration and mucin production. *Pancreatic cancer* - **Pancreatic adenocarcinoma** does show **significant perineural invasion** (present in 70-90% of cases) and is an important feature contributing to its poor prognosis and pain symptoms. - However, in the context of this question, **adenoid cystic carcinoma** is considered the **most characteristic** or **prototypical** example of perineural invasion, particularly among head and neck neoplasms. - Both are associated with perineural invasion, but adenoid cystic carcinoma is the textbook example. *Pleomorphic adenoma* - A **pleomorphic adenoma** is a benign mixed tumor of the salivary glands and usually does not exhibit **perineural invasion** [2]. - Malignant transformation into a carcinoma ex pleomorphic adenoma can occur, but the benign form primarily grows as an encapsulated mass [2]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Head and Neck, pp. 753-755. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Head and Neck, pp. 751-753.
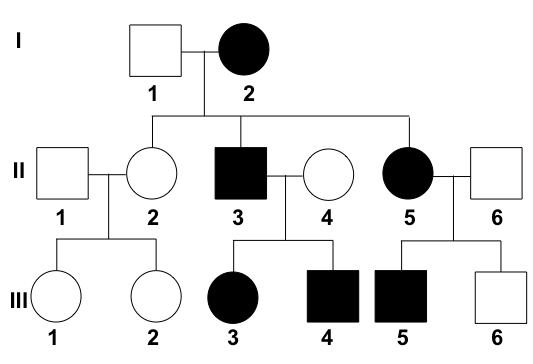
Question 8: What is the interpretation of the given pedigree chart?
- A. Autosomal dominant (Correct Answer)
- B. Incomplete penetrance
- C. Autosomal recessive
- D. X-linked dominant
Explanation: ***Autosomal dominant*** - The trait appears in **every generation**, indicated by affected individuals in the first, second, and third generations [1]. - Both males and females are affected relatively equally, and affected individuals transmit the trait to approximately half of their offspring, consistent with **vertical transmission** [1]. - **Male-to-male transmission** is present, which definitively rules out X-linked inheritance patterns [1]. *Incomplete penetrance* - This pattern would typically show some individuals who carry the disease-causing genotype but **do not express the phenotype** (unaffected). - In this pedigree, all individuals who are expected to express the trait based on the clear dominant pattern are indeed affected. *Autosomal recessive* - This mode of inheritance would typically show **skipped generations**, meaning affected individuals would often have unaffected parents who are carriers [1]. - In this chart, every affected individual has at least one affected parent, ruling out an autosomal recessive pattern [1]. X-linked dominant - In X-linked dominant inheritance, **no male-to-male transmission** would be observed, as fathers pass their X chromosome only to daughters. - The presence of affected males transmitting the trait to male offspring rules out this inheritance pattern. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 148-151.
Question 9: Identify the correct statement regarding Amyloidosis?
- A. Secondary amyloidosis is AL
- B. Amyloidosis is called so because of deposition of complex carbohydrates
- C. All of the options
- D. Amyloid deposits have beta pleated sheet conformation (Correct Answer)
Explanation: ### Amyloid deposits have beta-pleated sheet conformation - This **specific protein conformation** is characteristic of all amyloid fibrils, regardless of the precursor protein [1]. - The **beta-pleated sheet structure** is highly stable and resistant to enzymatic degradation, contributing to the pathologic accumulation of amyloid [1]. *Secondary amyloidosis is AL* - **Secondary amyloidosis (AA amyloidosis)** is caused by the deposition of **amyloid A protein**, which is derived from **serum amyloid A (SAA) protein** [3]. - **AL amyloidosis** is primary amyloidosis, resulting from the deposition of **immunoglobulin light chains** [2]. *Amyloidosis is called so because of deposition of complex carbohydrates* - The term "amyloid" was coined because early researchers mistakenly believed these deposits were **complex carbohydrates**, similar to starch [1]. - However, amyloidosis is actually characterized by the deposition of **abnormal proteins** that misfold and aggregate [1]. *All of the options* - This option is incorrect because the first two statements are factually inaccurate regarding the classification of amyloidosis and the composition of amyloid deposits. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of the Immune System, pp. 264-266. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of the Immune System, pp. 266-267. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 136-140.
Question 10: Match the following columns A. Caplan syndrome B. Mesothelioma C. Silicosis D. Asbestosis 1. Pleural effusion without shift 2. Crazy Paving 3. Lower lobe involved 4. Described in coal workers
- A. A4-B1-C3-D2 (Correct Answer)
- B. A4-B1-C3-D3
- C. A2-B1-C4-D3
- D. A4-B3-C1-D2
Explanation: ***A4-B1-C2-D3*** - **Caplan syndrome** is a rare lung condition characterized by the development of discrete **rheumatoid nodules** (0.5 to 5.0 cm in diameter) in the lungs of individuals with **rheumatoid arthritis** who also have a history of exposure to coal dust, thus it is described in **coal workers (A4)** [3], [4]. - **Mesothelioma** is an aggressive cancer arising from the lining of the lungs and abdomen, with hallmark features of **pleural effusion** without a mediastinal shift due to pleural encasement. It is strongly associated with **asbestos exposure (B1)** [2]. - **Silicosis** is a form of pneumoconiosis caused by the inhalation of crystalline silica. It characteristically causes fibrosis in the **upper and mid lung zones** [1]. The **"crazy paving" pattern** can be seen when silicosis is complicated by secondary **pulmonary alveolar proteinosis (PAP)**, making C2 the correct association. - **Asbestosis** is a chronic lung disease caused by inhaling asbestos fibers. It typically causes fibrosis in the **lower lobes** of the lungs, as asbestos fibers tend to accumulate in these areas due to gravity and ventilation patterns **(D3)** [1]. *A2-B1-C4-D3* - This option incorrectly associates "crazy paving" with asbestosis (D2 interpretation error) and incorrectly describes silicosis as primarily described in coal workers (C4), while silicosis is specifically due to silica exposure, not coal dust (though coal workers can develop silicosis from silica in coal mines). *A4-B3-C1-D2* - This option incorrectly states that mesothelioma primarily causes lower lobe involvement (B3), whereas its defining feature is pleural effusion without shift. - It also misidentifies pleural effusion without shift as a feature of silicosis (C1) and crazy paving as characteristic of asbestosis (D2). *A4-B1-C3-D3* - This option has a fundamental error: both silicosis (C) and asbestosis (D) are matched to feature 3 (lower lobe), which is impossible in a matching question. - Medically, silicosis affects **upper lobes**, not lower lobes, making this matching incorrect [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 698-699. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 339-340. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 331-332. [4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 333-334.