All (147)Anatomy (10)Anesthesiology (2)Biochemistry (10)Community Medicine (4)Dermatology (7)ENT (2)Forensic Medicine (3)Internal Medicine (19)Microbiology (8)Obstetrics and Gynecology (11)Ophthalmology (4)Orthopaedics (3)Pathology (12)Pediatrics (8)Pharmacology (16)Physiology (10)Psychiatry (3)Radiology (3)Surgery (12)
Q31
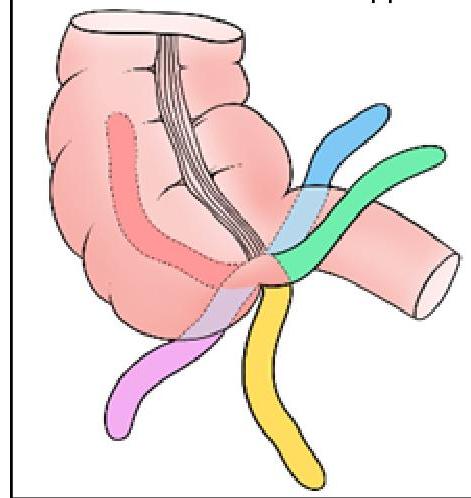
Identify the position of the appendix marked in BLACK in the given image:
Q32
What is the incorrect statement?
