All (147)Anatomy (10)Anesthesiology (2)Biochemistry (10)Community Medicine (4)Dermatology (7)ENT (2)Forensic Medicine (3)Internal Medicine (19)Microbiology (8)Obstetrics and Gynecology (11)Ophthalmology (4)Orthopaedics (3)Pathology (12)Pediatrics (8)Pharmacology (16)Physiology (10)Psychiatry (3)Radiology (3)Surgery (12)
Q21
What can cause the absence of fructose in seminal fluid?
Q22
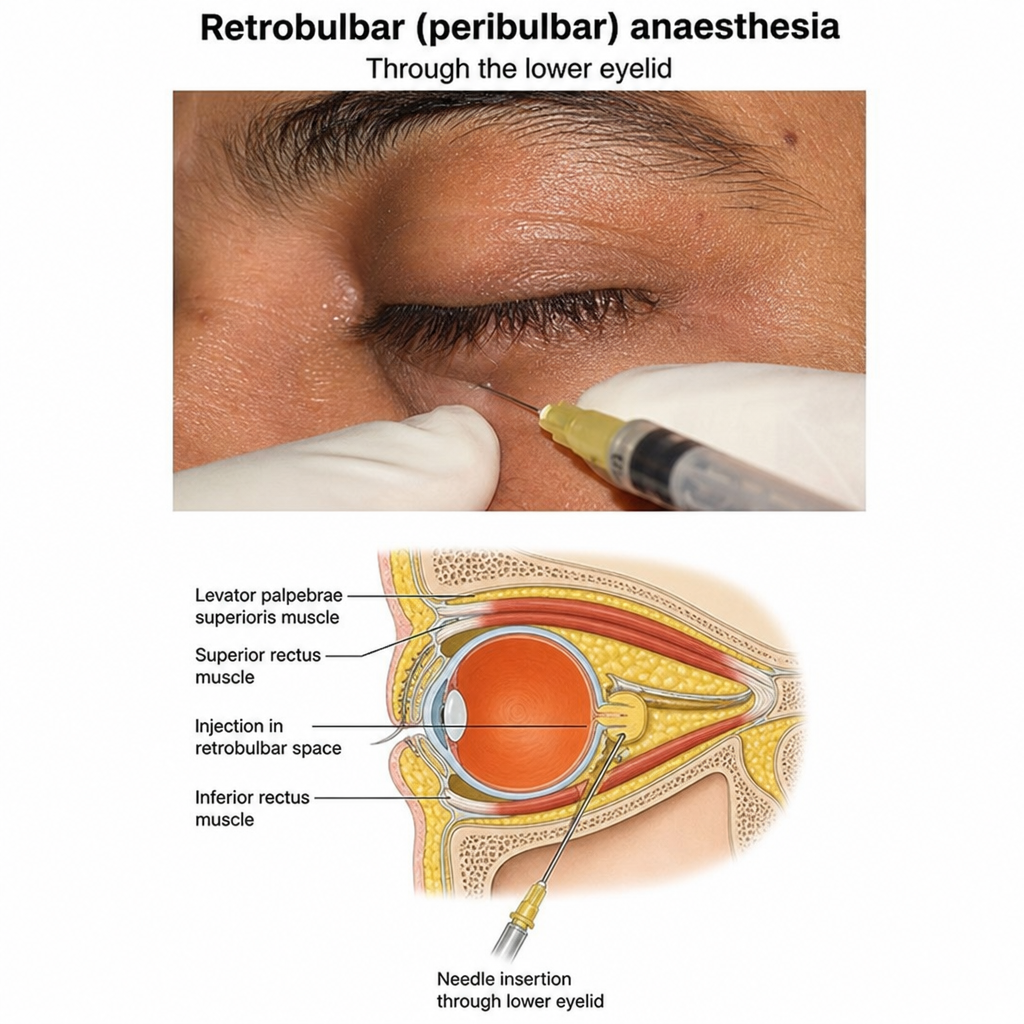
Which nerve is blocked in the image given below?