All (147)Anatomy (10)Anesthesiology (2)Biochemistry (10)Community Medicine (4)Dermatology (7)ENT (2)Forensic Medicine (3)Internal Medicine (19)Microbiology (8)Obstetrics and Gynecology (11)Ophthalmology (4)Orthopaedics (3)Pathology (12)Pediatrics (8)Pharmacology (16)Physiology (10)Psychiatry (3)Radiology (3)Surgery (12)
Q131
Which of the following structures is supplied by the superior gluteal nerve?
Q132
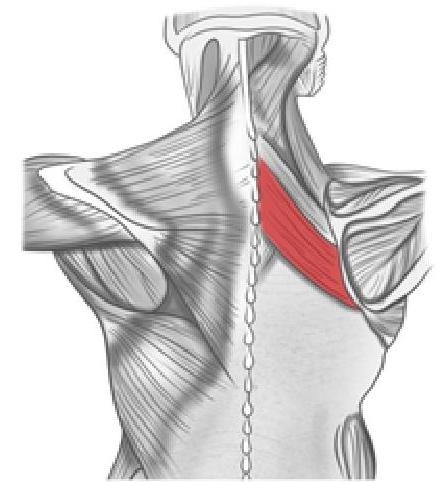
What is the action of the muscle shown in the image below?
Q133
Match the following: A) Glossopharyngeal nerve B) Spinal accessory nerve C) Facial nerve D) Mandibular nerve 1) Shrugging of shoulder 2) Touch sensation from the posterior one-third of the tongue 3) Chewing 4) Taste from the anterior two-thirds of the tongue