All (147)Anatomy (10)Anesthesiology (2)Biochemistry (10)Community Medicine (4)Dermatology (7)ENT (2)Forensic Medicine (3)Internal Medicine (19)Microbiology (8)Obstetrics and Gynecology (11)Ophthalmology (4)Orthopaedics (3)Pathology (12)Pediatrics (8)Pharmacology (16)Physiology (10)Psychiatry (3)Radiology (3)Surgery (12)
Q101
Arrange the following parts of sarcomere from periphery to center. 1. Z line 2. M line 3. A band 4. H zone
Q102
Blood pressure changes in radial artery were measured. Which of the following is the reason for initial rise in BP while performing Valsalva maneuver?
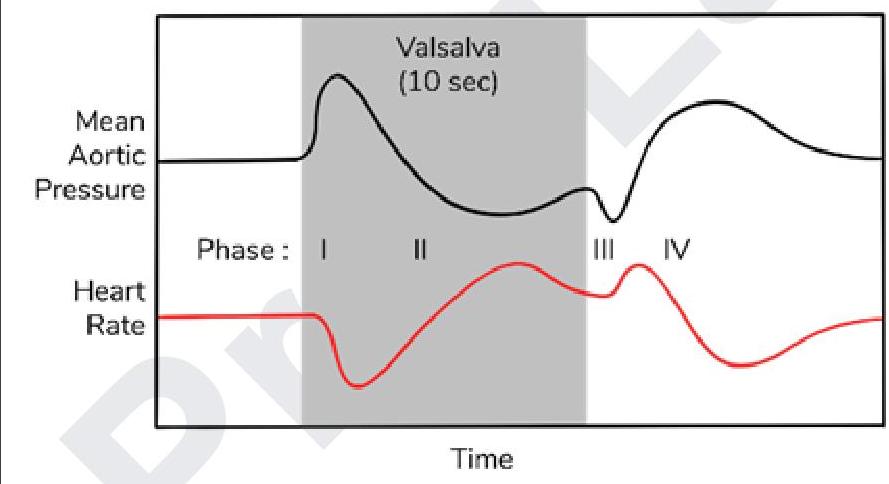
Q103
Assertion: RMP depends on proteins and phosphate ions. Reason: Diffusion potential can be calculated using nernst equation. Choose the best statement regarding the assertion and reason.
Q104
CO poisoning causes which type of hypoxia?