All SubjectsAnatomy (10)Anesthesiology (2)Biochemistry (10)Community Medicine (4)Dermatology (7)ENT (2)Forensic Medicine (3)Internal Medicine (19)Microbiology (8)Obstetrics and Gynecology (11)Ophthalmology (4)Orthopaedics (3)Pathology (12)Pediatrics (8)Pharmacology (16)Physiology (10)Psychiatry (3)Radiology (3)Surgery (12)
Q11
A 35-year-old female presents with skin thickening and muscle weakness. Her peripheries became pale on exposure to cold. Her ANA is positive and creatine kinase is increased. Scl-70 is positive and perifascicular infiltration is noted in biopsy. What is the antibody associated with this condition?
Q12
What is the possible cause of irreversible dementia?
Q13
What is the correct order for cardiac auscultation on the left side, from superior to inferior? a. Pulmonary b. Tricuspid c. Mitral
Q14
Match the following: A) Caplan syndrome- 1) Found first in coal worker B) Asbestosis- 2) Upper lobe predominance C) Mesothelioma- 3) Involves lower lobe D) Sarcoidosis- 4) Pleural effusion is seen
Q15
A patient presented with complaints of pain in the flank region with hematuria. On investigation, X-ray shows multiple calcification (stones) in both kidneys. What is the probable diagnosis?
Q16
KEYNOTE-189 trial for pembrolizumab is done for?
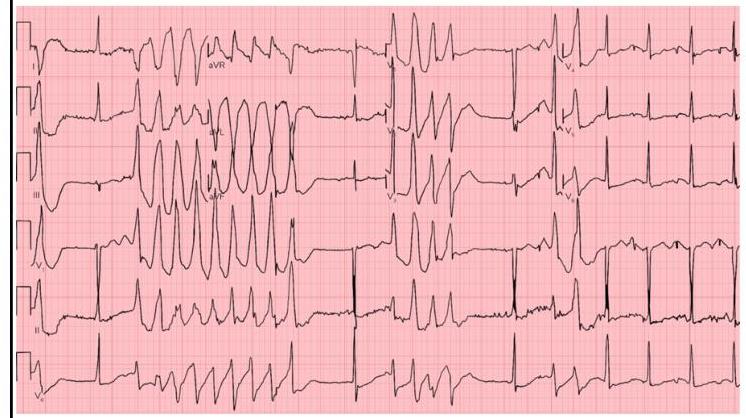
Q17
Identify the ECG given below?
Q18
Which of the following describes aortic regurgitation murmur?
Q19
All of the following are the causes of High output cardiac failure, except?