INI-CET 2022 — Physiology
11 Previous Year Questions with Answers & Explanations
Which physiological adaptation does not happen at high altitudes?
The countercurrent mechanism is present in which of the following parts of the body? A. Eye B. Testes C. Kidney D. Gut E. Lungs
What does zero pressure indicate in the pressure-volume curve?
The graph below shows oxygen dissociation curves. What does the curve marked as 'A' indicate?
What is the ratio of T cells to B cells in a healthy adult?
During polysomnography, which stage of sleep is represented by the marked areas when observing the following wave patterns? EOG (Electrooculography) EEG (Electroencephalography) EMG (Electromyography)
Which among the following organs has the least arteriovenous oxygen difference?
Which of the following is the primary tissue dependent on insulin for glucose uptake?
What is the normal insensible water loss?
A woman must vomit whenever she eats spicy food. Arrange the sequence of events during vomiting. 1. LES is open and UES is closed 2. Strong contractions in the stomach 3. Inspiration against a closed glottis 4. Relaxation of the pyloric sphincter 5. LES opens and UES opens 6. Reverse peristalsis in the small intestine LES: Lower esophageal sphincter UES: Upper esophageal sphincter
INI-CET 2022 - Physiology INI-CET Practice Questions and MCQs
Question 1: Which physiological adaptation does not happen at high altitudes?
- A. Pulmonary vasoconstriction
- B. Respiratory acidosis (Correct Answer)
- C. Hypoxia
- D. Polycythemia
Explanation: ***Respiratory acidosis*** - At high altitudes, the primary physiological response to **hypoxia** is to increase ventilation, leading to a decrease in **arterial PCO2**. - This reduction in **PCO2** causes **respiratory alkalosis**, not acidosis, as the body tries to compensate for the lower oxygen levels. *Pulmonary vasoconstriction* - This is a significant physiological response to **hypoxia** at high altitudes, leading to an increase in **pulmonary artery pressure**. - Its purpose is to divert blood flow to better-ventilated areas of the lung, but it can also contribute to **pulmonary hypertension**. *Hypoxia* - Reduced **atmospheric pressure** at high altitudes directly results in a lower partial pressure of oxygen (**PO2**), leading to **hypoxia**. - This low **PO2** is the primary trigger for most other physiological adaptations seen at high altitudes. *Polycythemia* - Prolonged exposure to **hypoxia** stimulates the kidneys to release **erythropoietin (EPO)**, which in turn increases **red blood cell production**. - This adaptive increase in **red blood cell count** and **hemoglobin concentration** aims to enhance the oxygen-carrying capacity of the blood.
Question 2: The countercurrent mechanism is present in which of the following parts of the body? A. Eye B. Testes C. Kidney D. Gut E. Lungs
- A. A, B, C, D, E are correct
- B. B and C are correct (Correct Answer)
- C. B, C, D, E are correct
- D. A, B, C are correct
Explanation: ***B and C are correct*** - The **countercurrent mechanism** is a biological process where two fluids flow in opposite directions across a semipermeable membrane or in close proximity to maximize exchange efficiency. - **Testes (B)**: The **pampiniform plexus** of veins surrounds the testicular artery, creating a countercurrent heat exchange system. Warm arterial blood descending to the testes is cooled by cooler venous blood ascending from the testes, maintaining the 2-3°C lower temperature required for optimal spermatogenesis. - **Kidney (C)**: The **loop of Henle** and **vasa recta** employ countercurrent multiplication and countercurrent exchange mechanisms to establish and maintain the corticomedullary osmotic gradient, which is essential for concentrating urine. *A, B, C, D, E are correct* - **Eye (A)**: The eye does not have a well-established countercurrent mechanism. Aqueous humor circulation and retinal blood flow do not operate on countercurrent principles. - **Gut (D)**: While intestinal villi have circulation, countercurrent exchange is not a primary or well-established mechanism in standard physiology teaching for the gut. - **Lungs (E)**: The lungs use **concurrent flow**, not countercurrent exchange. Pulmonary capillary blood and alveolar air flow in the same direction, which is less efficient than countercurrent but still allows adequate gas exchange. *A and B are correct* - This option incorrectly includes **Eye (A)**, which does not have a countercurrent mechanism. - It also excludes the **Kidney (C)**, which is one of the most classic and well-taught examples of countercurrent mechanisms in physiology. *A, B, C are correct* - This option incorrectly includes **Eye (A)**, which does not have a countercurrent mechanism. - While it correctly includes testes and kidney, the inclusion of the eye makes this medically inaccurate. *B, C, D, E are correct* - While **Testes (B)** and **Kidney (C)** definitely have countercurrent mechanisms, the inclusion of **Gut (D)** and **Lungs (E)** is incorrect. - The lungs specifically use concurrent, not countercurrent, gas exchange - this is a fundamental concept in respiratory physiology. - Countercurrent exchange in the gut is not a standard teaching point in medical physiology.
Question 3: What does zero pressure indicate in the pressure-volume curve?
- A. Functional residual capacity (Correct Answer)
- B. Inspiratory reserve volume
- C. Tidal volume
- D. Residual volume
Explanation: ***Functional residual capacity*** - This is the lung volume at which the **elastic recoil of the lungs** exactly balances the **elastic recoil of the chest wall**, resulting in zero net pressure across the respiratory system. - At **functional residual capacity (FRC)**, there is no airflow, and the **alveolar pressure equals atmospheric pressure (zero)**, indicating the equilibrium point. - Note: The **transpulmonary pressure remains positive** at FRC (approximately +5 cm H₂O), which keeps the lungs inflated against their elastic recoil. *Inspiratory reserve volume* - This is the **extra volume of air** that can be forcibly inhaled after a normal inspiration. - It involves active inspiration and therefore is associated with a **negative intrathoracic pressure**, not zero pressure. *Tidal volume* - This is the **volume of air inhaled and exhaled** during a normal quiet breathing cycle. - While breathing, pressures fluctuate, and the respiratory system is not at an equilibrium point of **zero pressure** throughout the tidal breath. *Residual volume* - This is the **volume of air remaining in the lungs** after a maximal exhalation. - The chest wall's outward recoil is greater than the lung's inward recoil at this point, resulting in a **negative intrapleural pressure** to keep the lungs from collapsing.
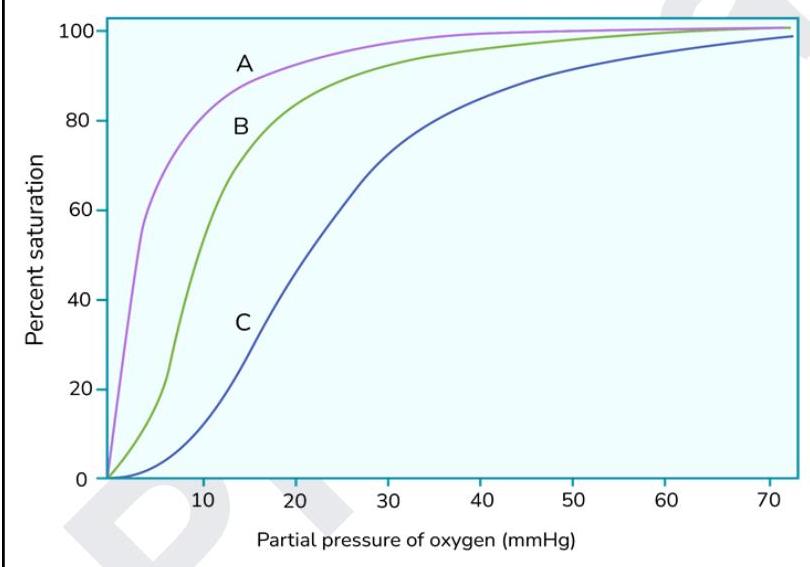
Question 4: The graph below shows oxygen dissociation curves. What does the curve marked as 'A' indicate?
- A. Myoglobin (Correct Answer)
- B. Methemoglobin
- C. Carboxyhemoglobinemia
- D. Fetal hemoglobin
Explanation: ***Myoglobin*** - Curve A shows a **hyperbolic oxygen dissociation curve** which is characteristic of myoglobin, indicating high oxygen affinity even at low partial pressures. - Myoglobin has only one heme group, allowing it to bind a single oxygen molecule with high affinity to **store oxygen in muscles**. *Methemoglobin* - Methemoglobin has a **ferric (Fe3+) iron** in its heme group, which cannot bind oxygen, thus reducing the overall oxygen-carrying capacity. - It would typically cause a **left shift** of the remaining functional hemoglobin's dissociation curve due to increased oxygen affinity, but this isn't directly represented as curve A's primary characteristic. *Carboxyhemoglobinemia* - **Carbon monoxide (CO)** binds to hemoglobin with a much higher affinity than oxygen, forming carboxyhemoglobin. - This binding leads to a **left shift** in the oxygen dissociation curve of the remaining functional hemoglobin and a decreased oxygen-carrying capacity, but curve A represents a species with inherently higher oxygen affinity. *Fetal hemoglobin* - Fetal hemoglobin (HbF) has a **higher affinity for oxygen** than adult hemoglobin (HbA), which is represented by a **left-shifted sigmoidal curve** compared to adult hemoglobin. - While it has higher affinity, its curve is still **sigmoidal**, unlike the hyperbolic curve of myoglobin (A).
Question 5: What is the ratio of T cells to B cells in a healthy adult?
- A. 3:1 (Correct Answer)
- B. 1:3
- C. 1:1
- D. 1:2
Explanation: ***3:1*** - In healthy adults, a typical peripheral blood sample shows a **predominance of T cells** over B cells. - This ratio reflects the differing roles and distributions of these lymphocytes; **T cells are more numerous** in circulation. *1:3* - This ratio would indicate **more B cells than T cells**, which is not typical for peripheral blood in a healthy individual. - An inversion of the usual T:B cell ratio could suggest certain disease states, such as specific **lymphoid malignancies**. *1:1* - While possible in some specific lymphoid tissues, a **1:1 ratio is not the standard** for circulating T and B cells in healthy adults. - This ratio would represent a **significantly higher proportion of B cells** than usually found in peripheral blood. *1:2* - This ratio implies **twice as many B cells as T cells**, which is significantly skewed compared to normal physiological levels in peripheral blood. - Such a high proportion of B cells is typically observed in states of **B-cell proliferation** or specific immune dysregulation.
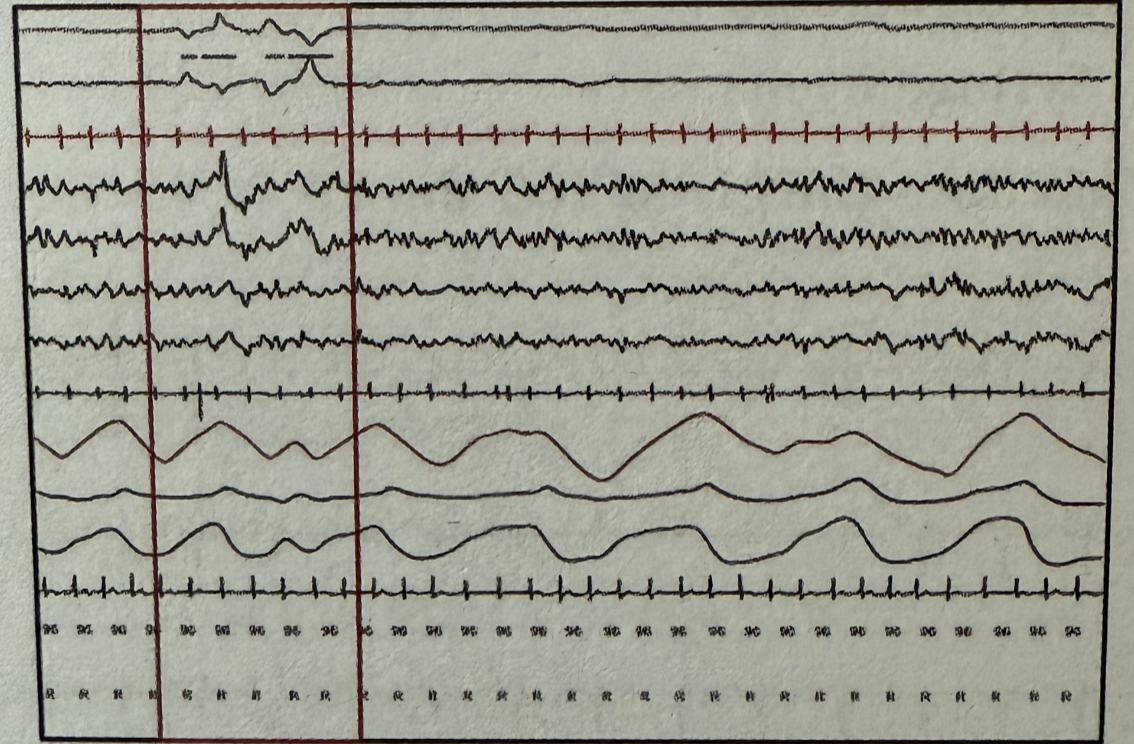
Question 6: During polysomnography, which stage of sleep is represented by the marked areas when observing the following wave patterns? EOG (Electrooculography) EEG (Electroencephalography) EMG (Electromyography)
- A. REM sleep
- B. NREM I sleep (Correct Answer)
- C. NREM II sleep
- D. NREM III sleep
Explanation: ***NREM I sleep*** - This stage is characterized by a transition from wakefulness to sleep, identifiable by the appearance of **slow eye movements** in the EOG and a reduction in EEG frequency with the presence of **theta waves**. - The EMG shows a decrease in muscle tone but without the complete atonia seen in REM sleep. *REM sleep* - **Rapid eye movements** are characteristic in the EOG, and the EEG shows **low-amplitude, mixed-frequency waves** similar to wakefulness. - The EMG would display profound muscle atonia, which is not evident in the provided tracing. *NREM II sleep* - This stage is marked by the presence of **sleep spindles** and **K-complexes** in the EEG, which are absent in the marked area. - Eye movements are generally absent, and muscle activity continues to be low. *NREM III sleep* - This is the deepest stage of sleep, characterized by **high-amplitude, slow-delta waves** (20-50% of the epoch) in the EEG. - Eye movements are typically absent, and muscle tone is very low but not completely absent.
Question 7: Which among the following organs has the least arteriovenous oxygen difference?
- A. Liver
- B. Skin
- C. Kidney (Correct Answer)
- D. Brain
Explanation: ***Kidney*** - The **kidney** has the lowest arteriovenous oxygen difference among these organs because its metabolic activity, relative to its blood supply, is designed for filtration rather than high oxygen extraction for work. - A significant portion of the kidney's oxygen consumption is related to **active transport** and **reabsorption**, but its unusually high blood flow (about 20-25% of cardiac output) ensures that the oxygen content of venous blood remains high. *Liver* - The liver receives a **dual blood supply** (hepatic artery and portal vein) and is highly metabolically active due to its roles in synthesis, detoxification, and nutrient processing, leading to a substantial oxygen extraction and thus a larger arteriovenous oxygen difference. - It has a significant oxygen demand for its numerous physiological functions, resulting in a lower oxygen content in its venous outflow compared to arterial blood. *Skin* - Skin blood flow is highly variable and plays a crucial role in **thermoregulation** in addition to metabolic needs. - While its baseline metabolic rate is moderate, its oxygen extraction can vary, but generally, it has a larger arteriovenous oxygen difference due to the oxygen demand of its various cellular layers and structures. *Brain* - The **brain** has a consistently high metabolic rate and continuous oxygen demand, consuming about 20% of the body's total oxygen at rest. - This consistent and high demand for oxygen results in a relatively large arteriovenous oxygen difference as it extracts a significant portion of oxygen from the arterial blood.
Question 8: Which of the following is the primary tissue dependent on insulin for glucose uptake?
- A. Adipose tissue
- B. Brain
- C. Muscle (Correct Answer)
- D. Pancreas
Explanation: ***Muscle (Correct Answer)*** - **Skeletal muscle** is the **primary insulin-dependent tissue** for glucose uptake, accounting for approximately **80-90% of insulin-stimulated glucose disposal** in the postprandial state. - Insulin promotes the translocation of **GLUT4 transporters** to the cell membrane in muscle cells, enabling rapid and substantial glucose uptake. - This makes muscle the most quantitatively significant site for insulin-mediated glucose clearance from the bloodstream. *Adipose tissue (Incorrect)* - While **adipose tissue** does exhibit insulin-dependent glucose uptake via **GLUT4 transporters**, its contribution to overall glucose disposal is **much smaller** compared to skeletal muscle. - Glucose uptake in adipocytes is important for **lipogenesis** and triglyceride storage, but represents only a minor fraction of total body insulin-stimulated glucose uptake. *Brain (Incorrect)* - The **brain** has a constant, high glucose requirement but utilizes **insulin-independent** glucose uptake mechanisms, primarily through **GLUT1 and GLUT3 transporters**. - Glucose uptake in the brain is regulated by **blood glucose concentration gradients**, not by insulin signaling. - This ensures continuous glucose supply to the brain regardless of insulin levels. *Pancreas (Incorrect)* - The **pancreas**, particularly beta cells, employs **insulin-independent** glucose uptake via **GLUT1 and GLUT2 transporters**. - These transporters function as **glucose sensors**, allowing beta cells to detect blood glucose levels and regulate insulin secretion accordingly. - The pancreas produces insulin but does not depend on insulin for its own glucose uptake.
Question 9: What is the normal insensible water loss?
- A. 150 mL/hour
- B. 50 mL/hour (Correct Answer)
- C. 200 mL/hour
- D. 100 mL/hour
Explanation: ***50 mL/hour*** - **Insensible water loss** occurs primarily through the **skin** and **respiratory tract** and typically amounts to approximately 1200 mL per day in an adult. - Dividing 1200 mL by 24 hours yields an average of **50 mL/hour**, representing normal physiological fluid loss not readily measurable. *150 mL/hour* - This value represents a significantly **elevated rate** of insensible water loss, which would suggest a patient experiencing **fever**, **tachypnea**, or a **hot environment**. - A sustained loss at this rate would quickly lead to **dehydration** if not compensated for by increased fluid intake. *200 mL/hour* - This is an **extreme rate** of water loss, indicating a severe condition such as **severe burns** affecting a large body surface area, **heat stroke**, or profound **hyperventilation**. - Such a high rate of fluid loss would be a medical emergency requiring aggressive fluid resuscitation. *100 mL/hour* - This rate of insensible water loss is **double the normal physiological rate** and, while not as extreme as 150 or 200 mL/hour, still implies increased metabolic activity or environmental stress. - It could be seen in individuals with moderate fever, increased physical activity, or in warmer ambient temperatures, and could contribute to mild dehydration over time.
Question 10: A woman must vomit whenever she eats spicy food. Arrange the sequence of events during vomiting. 1. LES is open and UES is closed 2. Strong contractions in the stomach 3. Inspiration against a closed glottis 4. Relaxation of the pyloric sphincter 5. LES opens and UES opens 6. Reverse peristalsis in the small intestine LES: Lower esophageal sphincter UES: Upper esophageal sphincter
- A. 4,6,2,1,3,5
- B. 4,6,2,5,3,1
- C. 6,4,2,5,1,3
- D. 6,4,2,3,1,5 (Correct Answer)
Explanation: ***6,4,2,3,1,5*** - The correct sequence of vomiting begins with **reverse peristalsis in the small intestine (6)**, which propels intestinal contents retrograde toward the stomach. - The **pyloric sphincter then relaxes (4)**, allowing duodenal contents to enter the stomach and mix with gastric contents. - **Strong stomach contractions (2)** follow, building initial pressure within the gastric lumen. - **Deep inspiration against a closed glottis (3)** is critical—this generates high intra-abdominal and intrathoracic pressure (the essential expulsive force). - The **LES opens while UES remains closed (1)**, allowing gastric contents to move into the esophagus. - Finally, the **UES opens (5)**, permitting expulsion of contents through the mouth. *4,6,2,1,3,5* - Incorrect because **pyloric sphincter relaxation precedes reverse peristalsis**, which is physiologically backwards—intestinal contents must first move toward the stomach before the pylorus can allow them entry. - The positioning of glottis closure late in the sequence misrepresents when intra-abdominal pressure is generated. *4,6,2,5,3,1* - This sequence incorrectly places **both sphincters opening (5) before the critical pressure-generating step (3)**, which would result in premature expulsion without adequate force. - The inspiration against closed glottis must occur before final sphincter opening to create the necessary expulsive pressure. *6,4,2,5,1,3* - This option misorders the final events by having **both sphincters open (5) before adequate pressure generation (3)** and before the sequential LES opening (1). - The glottis closure step is positioned too late—it must precede sphincter opening to generate the high intra-abdominal pressure required for forceful expulsion.