All SubjectsAnatomy (15)Anesthesiology (1)Biochemistry (8)Community Medicine (11)Dermatology (7)ENT (2)Forensic Medicine (7)Internal Medicine (16)Microbiology (13)Obstetrics and Gynecology (9)Ophthalmology (3)Orthopaedics (2)Pathology (16)Pediatrics (8)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (12)
Q11
A man was brought to the emergency room after poisoning with an unknown substance. Muscarinic poisoning was suspected and he was treated for the same. What is the possible presenting feature which led to the diagnosis?
Q12
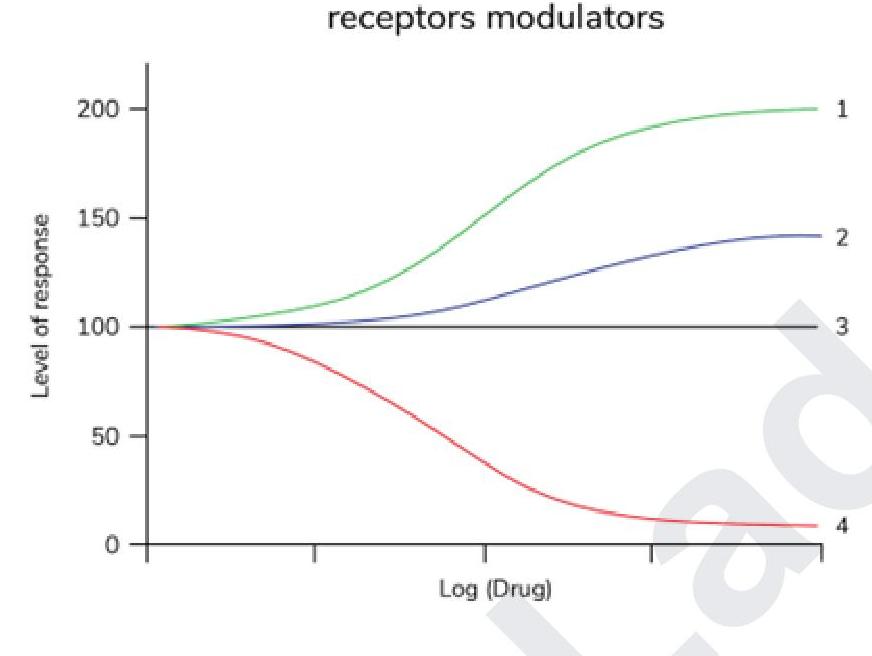
Which of the following statements is correct regarding the given graph?
Q13
Match the following antiarrhythmic drugs with their mechanism of action: | Mechanism of action | Drug | | :-- | :-- | | 1. Na+ channel blocker | A. Quinidine | | 2. K+ channel blocker | B. Digoxin | | 3. Na+K+ ATPase inhibitor | C. Esmolol | | 4. Beta-blocker | D. Ibutilide |
Q14
Match the following drugs with the targets of their actions: Drugs: A. Trastuzumab B. Infliximab C. Sirolimus D. Imatinib Targets: 1. BCR-ABL tyrosine kinase 2. mTOR 3. TNF alpha 4. HER2/neu