INI-CET 2022 — Pathology
11 Previous Year Questions with Answers & Explanations
A male patient with hemoptysis. On examination, hilar mass was present. The histopathological image is shown below. Immunohistochemistry revealed that the cells were positive for p40. What is the diagnosis?
The following is a histopathological image of thyroid pathology. What is the diagnosis?
Best method for the detection of mutations with low allele frequency is:
A baby is being evaluated for delayed developmental milestones. On examination, the child has hepatosplenomegaly. A microscopic image of the bone marrow evaluation is shown below. What is the most appropriate treatment?

Which of the following structures is pathognomonic for chromoblastomycosis?
The image below shows the life cycle of a virus. Which of the proteins of the virus act as oncogenes?
The Hb is 5 g/dL and the reticulocyte count is 9%. What is the corrected reticulocyte count?
Match the following cell types/patterns (Column A) with their associated malignancies (Column B): Column A (Cell types/patterns): a) Faggot cell b) Popcorn cell c) Starry sky pattern d) Cerebriform nuclei Column B (Associated malignancies): 1) Acute promyelocytic leukemia 2) Lymphocyte-predominant Hodgkin's lymphoma 3) Burkitt lymphoma 4) Sezary syndrome
A 35 year old woman presents with fatigue. Investigations revealed the following: Hb, 5 g/dL; MCH, 24; low MCV; leukocytes, 11,000/ uL, and platelets, 5 lakhs. The peripheral smear is shown below. What is the diagnosis? Normal values: - Mean cell volume (MCV); 90 ± 8 fL - Mean cell Hb(MCH); 30 ± 3 pg
Iron in tissues is stained by:
INI-CET 2022 - Pathology INI-CET Practice Questions and MCQs
Question 1: A male patient with hemoptysis. On examination, hilar mass was present. The histopathological image is shown below. Immunohistochemistry revealed that the cells were positive for p40. What is the diagnosis?
- A. Squamous cell carcinoma (Correct Answer)
- B. Adenocarcinoma lung
- C. Small cell carcinoma
- D. Large cell carcinoma
Explanation: ***Squamous cell carcinoma*** - The image displays features characteristic of **squamous cell carcinoma**, including nests of polygonal cells, prominent nucleoli, and areas of **keratinization** (forming keratin pearls) which are indicative of squamous differentiation [1]. - The positive immunohistochemistry staining for **p40** is a highly specific marker for squamous cell differentiation, further confirming the diagnosis in the context of a hilar mass and hemoptysis, which are common presentations for this type of lung cancer [2]. *Adenocarcinoma lung* - **Adenocarcinoma lung** typically presents with glandular differentiation, featuring structures like acini, tubules, or papillae, and often produces mucin, none of which are evident in the provided image [1]. - Immunohistochemically, adenocarcinoma would typically stain positive for **TTF-1** or **Napsin A**, and would be negative for p40. *Small cell carcinoma* - **Small cell carcinoma** shows small, round to oval cells with scant cytoplasm, finely granular chromatin (salt and pepper pattern), and frequent mitoses with extensive necrosis [3]. - These cells are much smaller than squamous cells and lack keratinization. IHC would show positivity for **synaptophysin, chromogranin, and CD56** (neuroendocrine markers), not p40 [3]. *Large cell carcinoma* - **Large cell carcinoma** is a diagnosis of exclusion showing undifferentiated large cells without glandular or squamous differentiation features. - It lacks the keratinization and intercellular bridges seen here, and would be **p40 negative** as it shows no squamous differentiation. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 723-724. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 336-337. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 337-338.
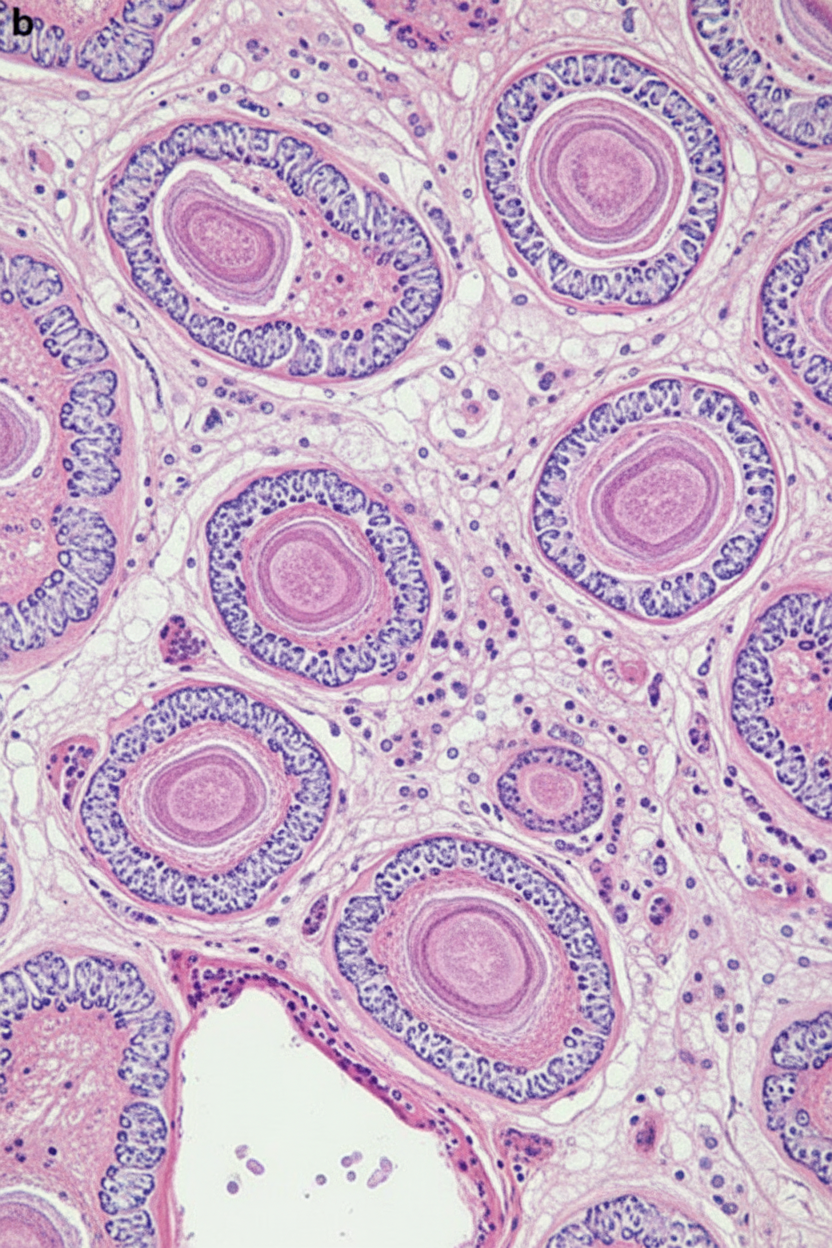
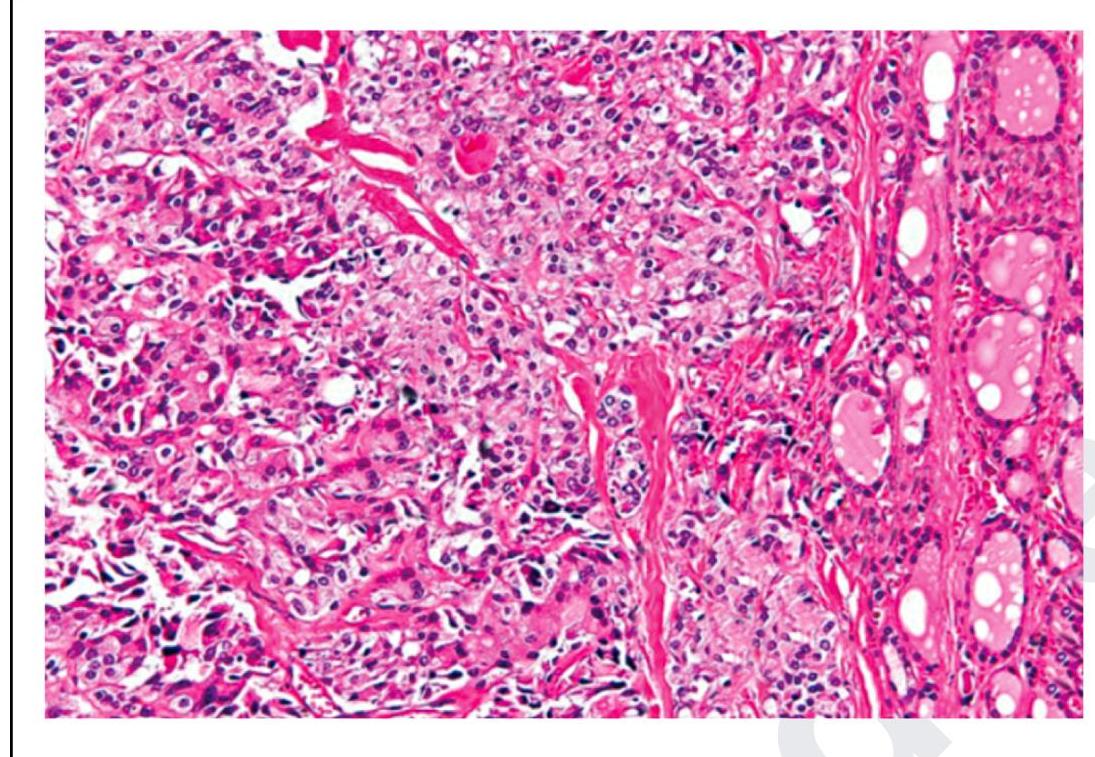
Question 2: The following is a histopathological image of thyroid pathology. What is the diagnosis?
- A. Papillary carcinoma of thyroid
- B. Medullary carcinoma of thyroid (Correct Answer)
- C. Follicular carcinoma of thyroid
- D. Anaplastic carcinoma of thyroid
Explanation: ***Medullary carcinoma of thyroid*** - This image shows sheets and nests of **polygonal to spindle-shaped cells**, which are characteristic of medullary thyroid carcinoma, especially when mixed with an **amyloid stroma** (seen as amorphous eosinophilic material) [2]. - The presence of **neuroendocrine features** and the production of **calcitonin** are hallmarks of these C-cell tumors [1], [2]. *Papillary carcinoma of thyroid* - Characterized by **papillary architecture**, **ground-glass (Orphan Annie eye) nuclei**, nuclear grooves, and intranuclear cytoplasmic inclusions. - These features are not prominently seen in the provided image. *Follicular carcinoma of thyroid* - Defined by an invasive growth pattern of **well-differentiated follicular cells** forming follicles, with either capsular or vascular invasion [2]. - The image does not show classic follicular architectural patterns or clear evidence of invasion in the absence of a capsule. *Anaplastic carcinoma of thyroid* - This is a highly aggressive and undifferentiated tumor with **marked pleomorphism**, bizarre giant cells, and high mitotic activity [2]. - While there is some pleomorphism, the overall pattern and cellular morphology in the image are more consistent with medullary carcinoma than the extreme anaplasia. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1102-1103. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 428-431.
Question 3: Best method for the detection of mutations with low allele frequency is:
- A. FISH
- B. Droplet digital PCR (Correct Answer)
- C. Sanger sequencing
- D. Nested PCR
Explanation: ***Droplet digital PCR*** - **Droplet digital PCR (ddPCR)** offers superior sensitivity for detecting **low allele frequency mutations** by partitioning the sample into thousands of individual reactions. - This compartmentalization allows for the direct quantification of target DNA molecules without relying on a standard curve, making it highly accurate for rare mutation detection. *FISH* - **Fluorescence in situ hybridization (FISH)** primarily detects **chromosomal abnormalities** like translocations, deletions, or amplifications, rather than single-nucleotide variants or small indels with low allele frequencies [2]. - It visualizes genetic changes at a **cytogenetic level** on an intracellular basis, not typically for quantifying rare DNA mutations in a heterogeneous sample. *Sanger sequencing* - **Sanger sequencing** is the gold standard for **sequencing individual DNA fragments** but has a detection limit of around 15-20% for allele frequency, making it unsuitable for very low allele frequency mutations [1]. - It struggles to reliably detect minor alleles when they are present in a small proportion of the total DNA pool. *Nested PCR* - **Nested PCR** increases the sensitivity and specificity of amplification by using two sets of primers in a sequential manner but does not inherently provide the **quantification capability** or the same level of **low allele frequency detection** as ddPCR processes. - While sensitive for detecting target sequences, it is not designed for precise quantification of rare mutations in a background of wild-type sequences. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, p. 185. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 185-186.
Question 4: A baby is being evaluated for delayed developmental milestones. On examination, the child has hepatosplenomegaly. A microscopic image of the bone marrow evaluation is shown below. What is the most appropriate treatment?
- A. Macrolides for 4 months
- B. Steroid irrigation and antihistamines
- C. Repeat surgery
- D. Biological therapy (Correct Answer)
Explanation: ***Biological therapy*** - The image likely shows a **Gaucher cell** (macrophage engorged with glucocerebroside, characterized by a "crinkled paper" or "crumpled tissue paper" cytoplasm) [1]. This is pathognomonic for **Gaucher disease**, which presents with **hepatosplenomegaly** and **developmental delay** in infants. - The standard treatment for Gaucher disease is **enzyme replacement therapy (ERT)**, which is a form of biological therapy replacing the deficient glucocerebrosidase enzyme [2]. *Macrolides for 4 months* - Macrolides are a class of **antibiotics** used to treat bacterial infections. - They are not indicated for lysosomal storage disorders like Gaucher disease, which is a **genetic metabolic disorder** [2]. *Steroid irrigation and antihistamines* - This treatment regimen is typically associated with allergic conditions or localized inflammatory responses, such as **allergic rhinitis** or **sinusitis**. - It bears no relevance to the systemic accumulation of lipids seen in Gaucher disease. *Repeat surgery* - While splenectomy was historically performed for massive splenomegaly in Gaucher disease, it does not address the underlying metabolic defect or systemic manifestations. - Furthermore, this case does not suggest a previous surgical intervention that requires repeating, and surgery is not the primary treatment for the metabolic disorder itself. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, pp. 162-163. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Genetic Disorders, p. 159.
Question 5: Which of the following structures is pathognomonic for chromoblastomycosis?
- A. Asteroid body
- B. Sclerotic body (Correct Answer)
- C. Budding yeast
- D. Negri body
Explanation: ***Sclerotic body*** - **Sclerotic bodies**, also known as **Medlar bodies** or **fumagoid cells**, are characteristic coin-shaped, thick-walled, septate, dematiaceous structures observed histologically in affected tissues. - Their presence is **pathognomonic** for chromoblastomycosis, a chronic fungal infection of the skin and subcutaneous tissue. *Asteroid body* - **Asteroid bodies** are typically found in **sporotrichosis**, representing an antigen-antibody complex surrounding fungal elements. - They are not characteristic of chromoblastomycosis. *Budding yeast* - **Budding yeast** forms are commonly seen in various fungal infections, such as **candidiasis** or **cryptococcosis**, but are not specific to chromoblastomycosis. [1] - This morphology indicates yeast proliferation but lacks the distinctive sclerotic appearance. *Negri body* - **Negri bodies** are eosinophilic, sharply demarcated neuronal cytoplasmic inclusions found in the diagnostic examination of **rabies** infection. - They are entirely unrelated to fungal infections like chromoblastomycosis. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, p. 717.
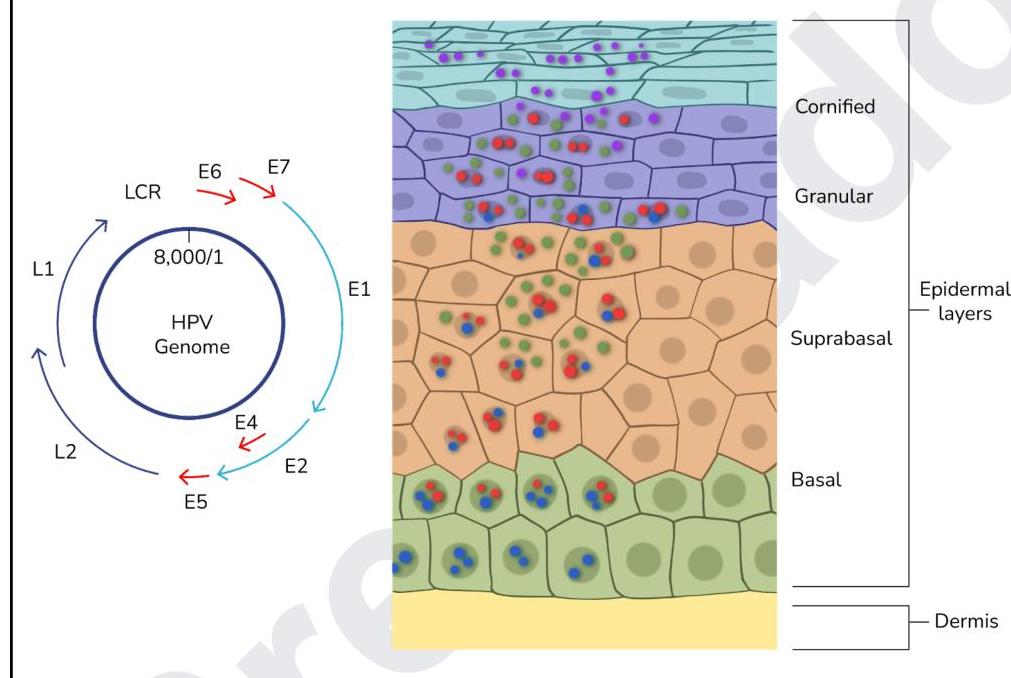
Question 6: The image below shows the life cycle of a virus. Which of the proteins of the virus act as oncogenes?
- A. L1, L2
- B. E1, E2, E5
- C. E1, E2
- D. E6, E7 (Correct Answer)
Explanation: ***E6, E7*** - The **E6** and **E7** proteins of high-risk human papillomaviruses (HPVs) are considered **oncogenes** because they interfere with critical tumor suppressor pathways [1][2]. - **E6** promotes the degradation of **p53**, a tumor suppressor protein, while **E7** inactivates **retinoblastoma protein (pRb)**, leading to uncontrolled cell proliferation and increased risk of malignant transformation [2]. *L1, L2* - **L1** and **L2** are **late proteins** (structural proteins) that form the **viral capsid** (outer shell) of the HPV virion. - They are essential for assembling new viral particles but do not directly contribute to the oncogenic process by disrupting host cell cycle regulation. *E1, E2, E5* - **E1** is involved in **viral DNA replication**, acting as a helicase and ATPase. - **E2** regulates **viral gene expression** and DNA replication, while **E5** is a small transmembrane protein that can contribute to cell growth but is generally considered less potent in oncogenesis than E6 and E7, and its exact role varies by HPV type. *E1, E2* - **E1** is critical for **viral DNA replication**, and **E2** regulates viral gene transcription and DNA replication. - While important for the viral life cycle, neither E1 nor E2 are the primary drivers of oncogenesis in the way E6 and E7 are, as they do not directly target key tumor suppressor proteins like p53 and pRb. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Female Genital Tract, pp. 1007-1008. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, pp. 334-335.
Question 7: The Hb is 5 g/dL and the reticulocyte count is 9%. What is the corrected reticulocyte count?
- A. 5
- B. 3 (Correct Answer)
- C. 1.8
- D. 4.5
Explanation: ***3*** - The **corrected reticulocyte count (CRC)** is calculated to adjust for varying degrees of anemia, providing a more accurate assessment of bone marrow erythropoietic activity. The formula is: **CRC = observed reticulocyte % × (patient's HCT / normal HCT)**. - Assuming a normal hematocrit (HCT) of 45% and a direct hemoglobin to hematocrit conversion of 1:3 for 5 g/dL Hb (so HCT = 15%), then CRC = 9% × (15/45) = 9% × 1/3 = **3%**. *5* - This value is likely obtained by an **incorrect calculation** or by applying an inappropriate correction factor. - It does not properly account for the **severity of anemia** in the calculation of the corrected reticulocyte count [2]. *1.8* - This result may represent confusion with the **Reticulocyte Production Index (RPI)**, which further corrects for premature reticulocyte release by dividing CRC by a maturation time factor (typically 1.5-2 in severe anemia) [1]. - However, the question specifically asks for the **corrected reticulocyte count**, not the RPI, making this an inappropriate over-correction. *4.5* - This value might be a result of **dividing the observed reticulocyte count by a factor of 2**, which is not the standard correction for anemia. - It does not accurately reflect the **bone marrow's response** to the severe anemic state. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 586-587. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 590-591.
Question 8: Match the following cell types/patterns (Column A) with their associated malignancies (Column B): Column A (Cell types/patterns): a) Faggot cell b) Popcorn cell c) Starry sky pattern d) Cerebriform nuclei Column B (Associated malignancies): 1) Acute promyelocytic leukemia 2) Lymphocyte-predominant Hodgkin's lymphoma 3) Burkitt lymphoma 4) Sezary syndrome
- A. 1-a, 2-d, 3-c, 4-b
- B. 1-b, 2-c, 3-a, 4-d
- C. 1-a, 2-b, 3-c, 4-d (Correct Answer)
- D. 1-b, 2-a, 3-d, 4-c
Explanation: ***1-a, 2-b, 3-c, 4-d*** - **Acute promyelocytic leukemia (APL)** is characterized by **faggot cells**, which are abnormal promyelocytes containing multiple **Auer rods**. - **Lymphocyte-predominant Hodgkin's lymphoma** is associated with **popcorn cells** (also known as L&H cells), which are large, multilobated Reed-Steinberg variant cells [3]. - **Burkitt lymphoma** shows the characteristic **starry sky pattern**, resulting from uniformly sized tumor cells interspersed with numerous tingible body macrophages [1]. - **Sézary syndrome** is characterized by **cerebriform nuclei** in Sézary cells, which are a hallmark of this leukemic variant of cutaneous T-cell lymphoma [2]. *1-a, 2-d, 3-c, 4-b* - This option incorrectly associates **cerebriform nuclei** with lymphocyte-predominant Hodgkin's lymphoma; this lymphoma is characterized by **popcorn cells**. - It also mismatches **Sézary syndrome** with popcorn cells; Sézary syndrome is defined by **cerebriform nuclei** [2]. *1-b, 2-c, 3-a, 4-c* - This option incorrectly links **popcorn cells** with acute promyelocytic leukemia; APL is characterized by **faggot cells** with Auer rods. - It also misassociates **Burkitt lymphoma** with faggot cells; Burkitt lymphoma shows the distinctive **starry sky pattern** [1]. *1-b, 2-a, 3-d, 4-c* - This option incorrectly matches **popcorn cells** with acute promyelocytic leukemia; APL contains **faggot cells** with multiple Auer rods. - It also wrongly associates **faggot cells** with lymphocyte-predominant Hodgkin's lymphoma; this condition features **popcorn cells** (L&H cells) [3]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, p. 606. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Diseases Of The Urinary And Male Genital Tracts, pp. 564-565. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of White Blood Cells, Lymph Nodes, Spleen, and Thymus, pp. 613-614, 616.
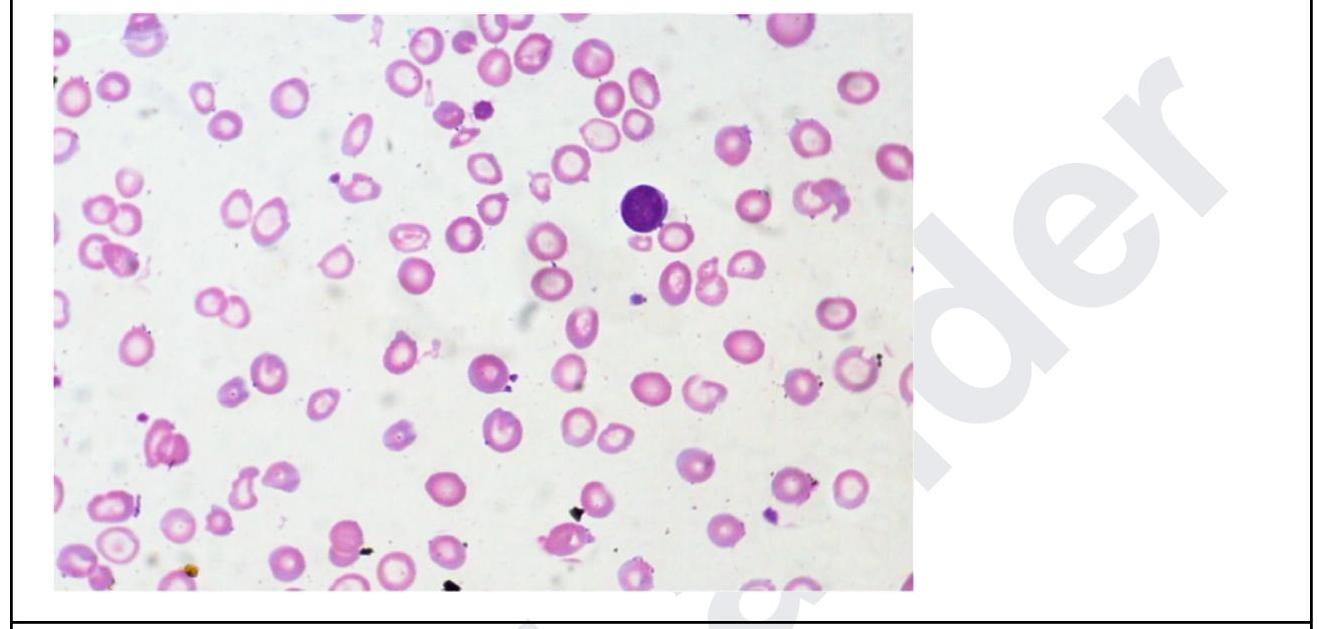
Question 9: A 35 year old woman presents with fatigue. Investigations revealed the following: Hb, 5 g/dL; MCH, 24; low MCV; leukocytes, 11,000/ uL, and platelets, 5 lakhs. The peripheral smear is shown below. What is the diagnosis? Normal values: - Mean cell volume (MCV); 90 ± 8 fL - Mean cell Hb(MCH); 30 ± 3 pg
- A. Essential thrombocytosis
- B. Iron - deficiency anemia (Correct Answer)
- C. Thalassemia major
- D. Megaloblastic anemia
Explanation: ***Iron-deficiency anemia*** - The patient presents with **severe anemia (Hb 5 g/dL)**, **low MCH (24 pg)**, and **low MCV**, which are classic indicators of **microcytic, hypochromic anemia** [3]. The peripheral smear shows **hypochromic microcytic red cells** with abundant central pallor and **anisopoikilocytosis**, consistent with iron-deficiency anemia [1]. - While the **platelet count is elevated (5 lakhs)**, it can occur in iron deficiency as reactive thrombocytosis [1]. Leukocytosis in the absence of infection may be a mild reactive process secondary to severe anemia. *Essential thrombocytosis* - This is a **myeloproliferative neoplasm** characterized by significantly elevated platelet counts (often > 450,000/uL), but typically does not present with severe anemia, low MCH, or low MCV. - The primary issue in this patient is severe anemia with microcytic hypochromic features, not isolated thrombocytosis. *Thalassemia major* - While thalassemia major also presents with **microcytic, hypochromic anemia** and can have a very low MCV, it usually manifests in early childhood and is associated with significant **hemolysis**, **splenomegaly**, and characteristic red blood cell morphology such as **target cells** and **nucleated red blood cells** [2]. - The extremely low Hb and microcytic indices alone are not enough to distinguish it from severe iron deficiency without further specific markers like iron studies or hemoglobin electrophoresis. *Megaloblastic anemia* - Megaloblastic anemia is characterized by **macrocytic anemia** (high MCV), which is the opposite of the low MCV presented in this case. - It typically results from **vitamin B12** or **folate deficiency** and the peripheral smear would show **macro-ovalocytes** and **hypersegmented neutrophils**, which are not seen here. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 590-591. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Red Blood Cell and Bleeding Disorders, p. 648. [3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Red Blood Cell and Bleeding Disorders, pp. 638-639.
Question 10: Iron in tissues is stained by:
- A. Masson's trichrome
- B. PAS
- C. Congo red
- D. Prussian blue (Correct Answer)
Explanation: ***Prussian blue*** - The **Prussian blue reaction**, also known as **Perls' stain**, specifically detects **ferric iron (Fe³⁺)** in tissues [3]. - It forms a **bright blue precipitate** (ferric ferrocyanide) when ferric iron reacts with potassium ferrocyanide in an acidic solution. *Masson's trichrome* - This stain is primarily used to differentiate **collagen fibers** from muscle fibers, which appear blue/green and red, respectively [1]. - It does not specifically stain or identify iron deposits in tissues. *PAS* - The **Periodic acid-Schiff (PAS) stain** is used to identify **carbohydrates** such as glycogen, mucosubstances, and fungal cell walls, which appear magenta. - It is not used for the detection of iron. *Congo red* - **Congo red** is a specialized stain used for identifying **amyloid deposits**, which appear pink-red and show apple-green birefringence under polarized light [2]. - It is not used for staining iron in tissues. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 25-26. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of the Immune System, pp. 268-269. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 394-395.