All (164)Anatomy (15)Anesthesiology (1)Biochemistry (8)Community Medicine (11)Dermatology (7)ENT (2)Forensic Medicine (7)Internal Medicine (16)Microbiology (13)Obstetrics and Gynecology (9)Ophthalmology (3)Orthopaedics (2)Pathology (16)Pediatrics (8)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (12)
Q51
A young man presents with skin lesions as shown in the image below. All of the following organisms can spread through dermal and subcutaneous lymphatics, except

Q52
Which virus can be identified by a PCR method and is endemic to India?
Q53
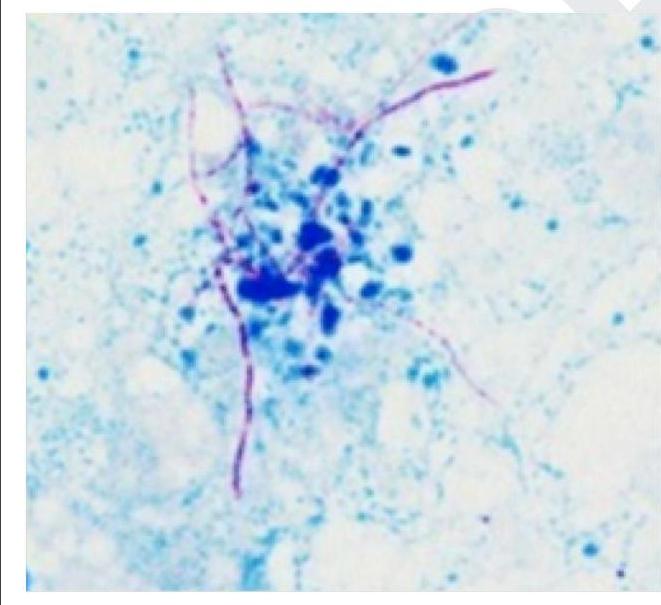
Which of the following is a gram-positive organism that shows the following appearance on Ziehl-Neelsen staining?
Q54
The following are parvovirus - related disease - population pairs. Identify the incorrect pair. 1. Aplastic anemia - Patient with hereditary hemolytic anemia 2. Non - immune hydrops - pregnant women 3. Erythema infectiosum - infants 4. Non - erosive arthritis - Patients of SLE
Q55
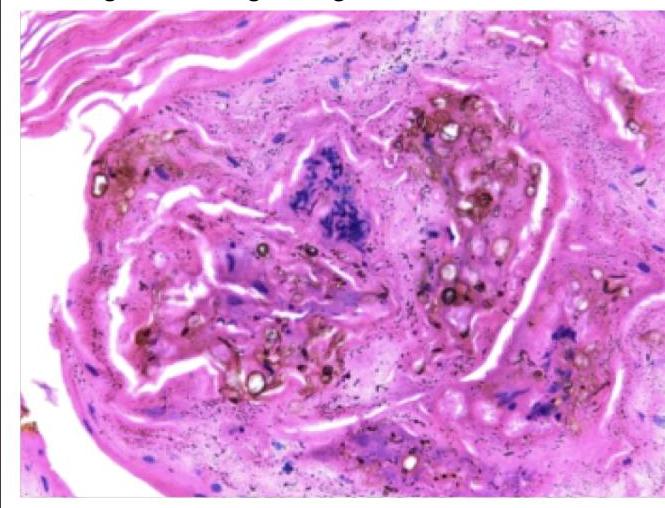
A forest worker developed skin lesions over the forearm, which initially started as macules but then became nodules. Histology of the nodule shows the following findings. Which of the following is true regarding this condition?
Q56
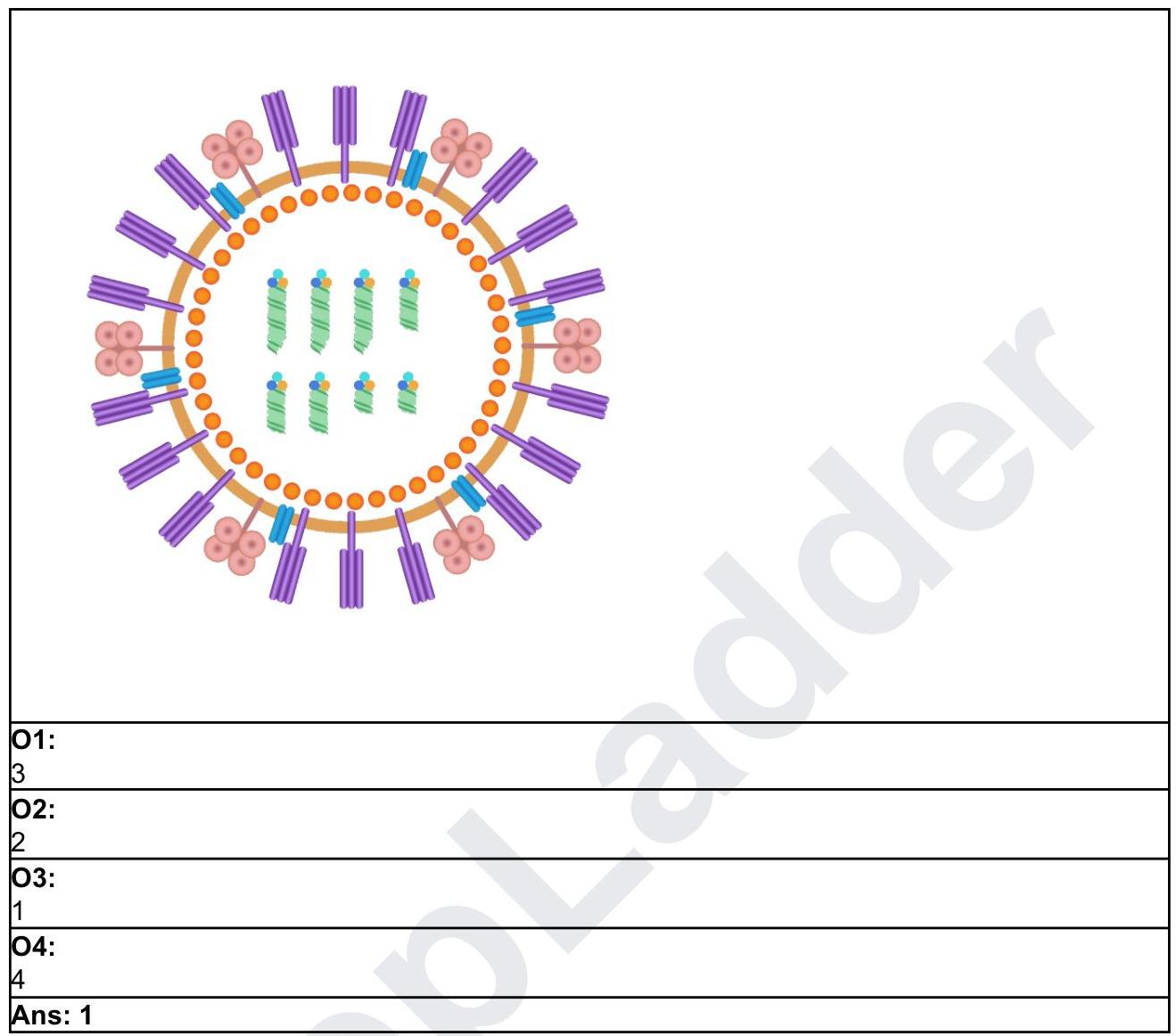
The viruses of the Filoviridae family like Ebola and Marburg resemble which of the following morphologies?