All (164)Anatomy (15)Anesthesiology (1)Biochemistry (8)Community Medicine (11)Dermatology (7)ENT (2)Forensic Medicine (7)Internal Medicine (16)Microbiology (13)Obstetrics and Gynecology (9)Ophthalmology (3)Orthopaedics (2)Pathology (16)Pediatrics (8)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (12)
Q41
Antigen presented on MHC class I molecules activates which of the following cells?
Q42
Which of the following is true about anti-CMV IgG antibodies?
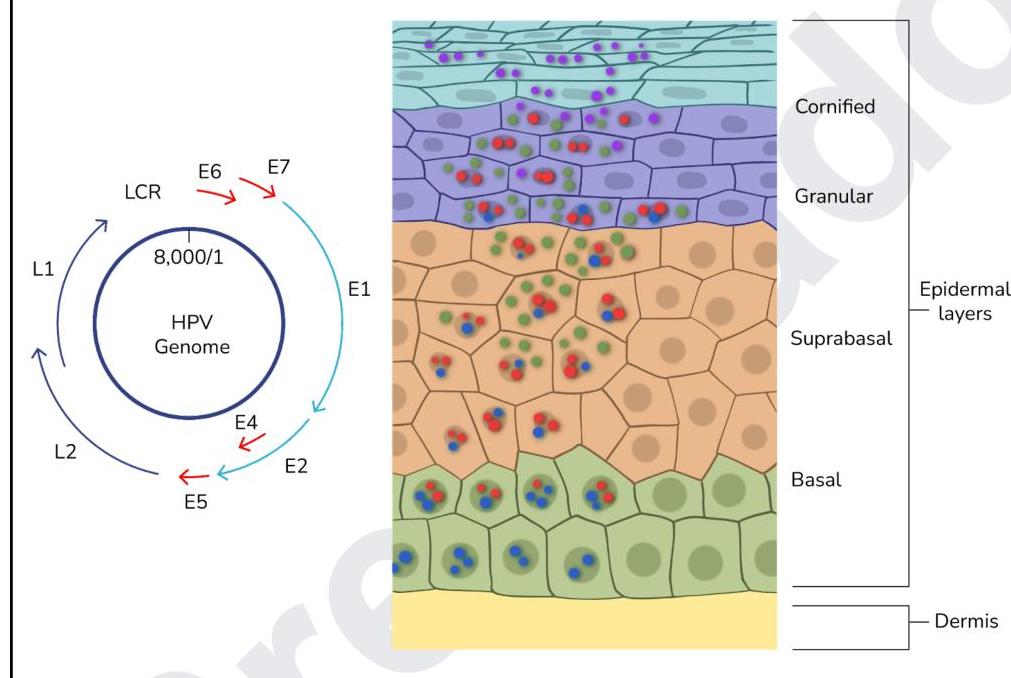
Q43
Which of the following statements regarding the given image is correct?
Q44
Which of the following are acid-fast staining organisms? 1. Nocardia 2. Mycobacterium leprae 3. Actinomyces 4. Cryptosporidium parvum 5. Isospora belli
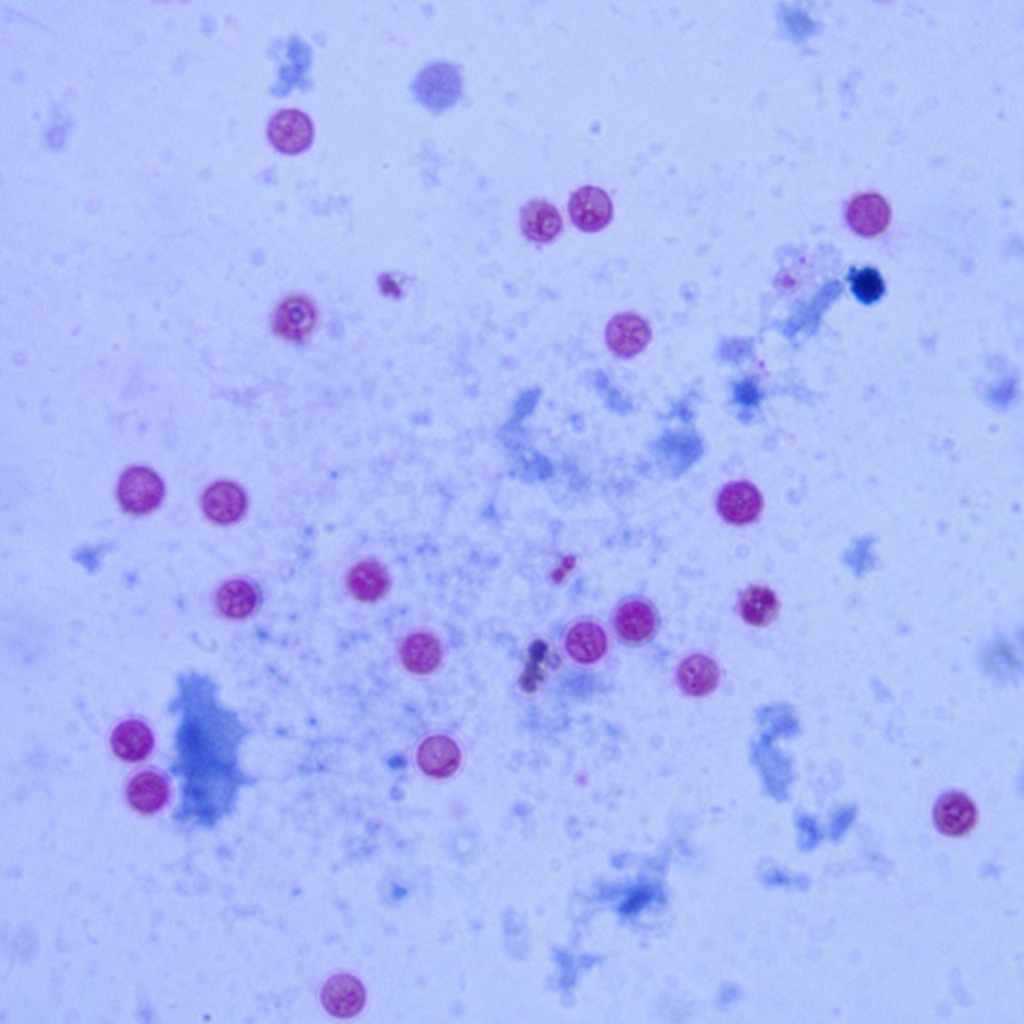
Q45
An HIV patient came to the clinic with a history of diarrhea. Stool microscopy showed the oocysts that were 4-6 µm in size. The image is shown below. Identify the organism.