All (164)Anatomy (15)Anesthesiology (1)Biochemistry (8)Community Medicine (11)Dermatology (7)ENT (2)Forensic Medicine (7)Internal Medicine (16)Microbiology (13)Obstetrics and Gynecology (9)Ophthalmology (3)Orthopaedics (2)Pathology (16)Pediatrics (8)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (12)
Q11
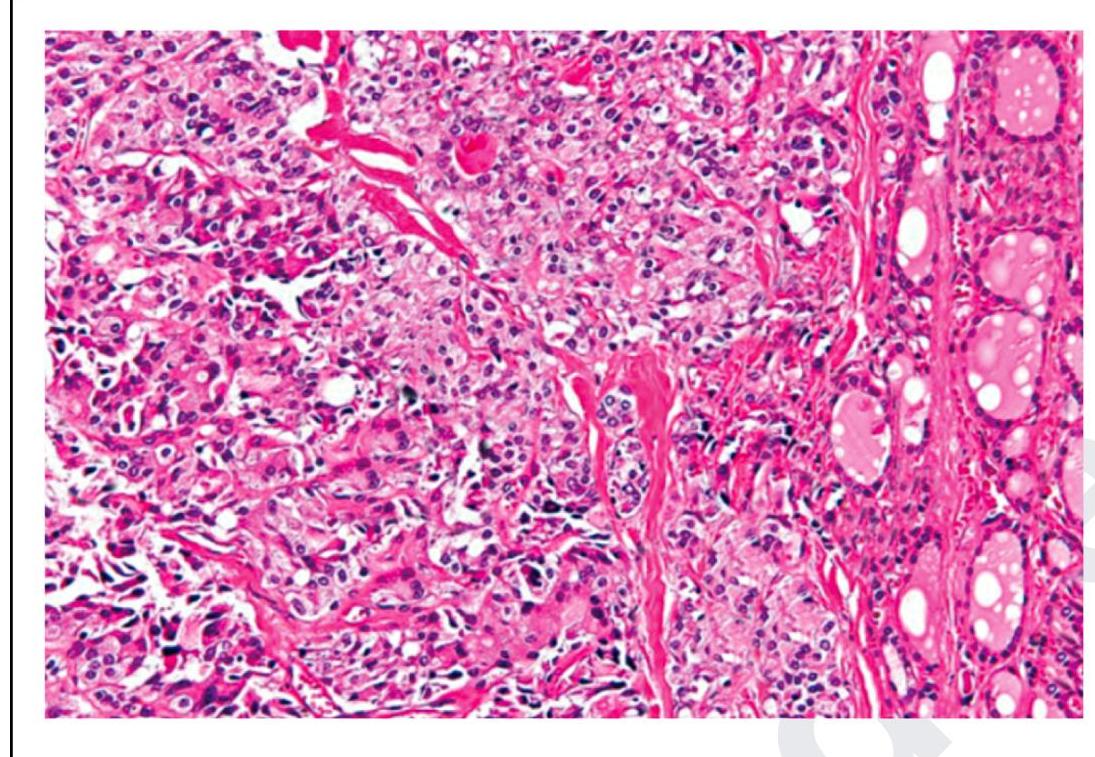
The following is a histopathological image of thyroid pathology. What is the diagnosis?