All (164)Anatomy (15)Anesthesiology (1)Biochemistry (8)Community Medicine (11)Dermatology (7)ENT (2)Forensic Medicine (7)Internal Medicine (16)Microbiology (13)Obstetrics and Gynecology (9)Ophthalmology (3)Orthopaedics (2)Pathology (16)Pediatrics (8)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (12)
Q151
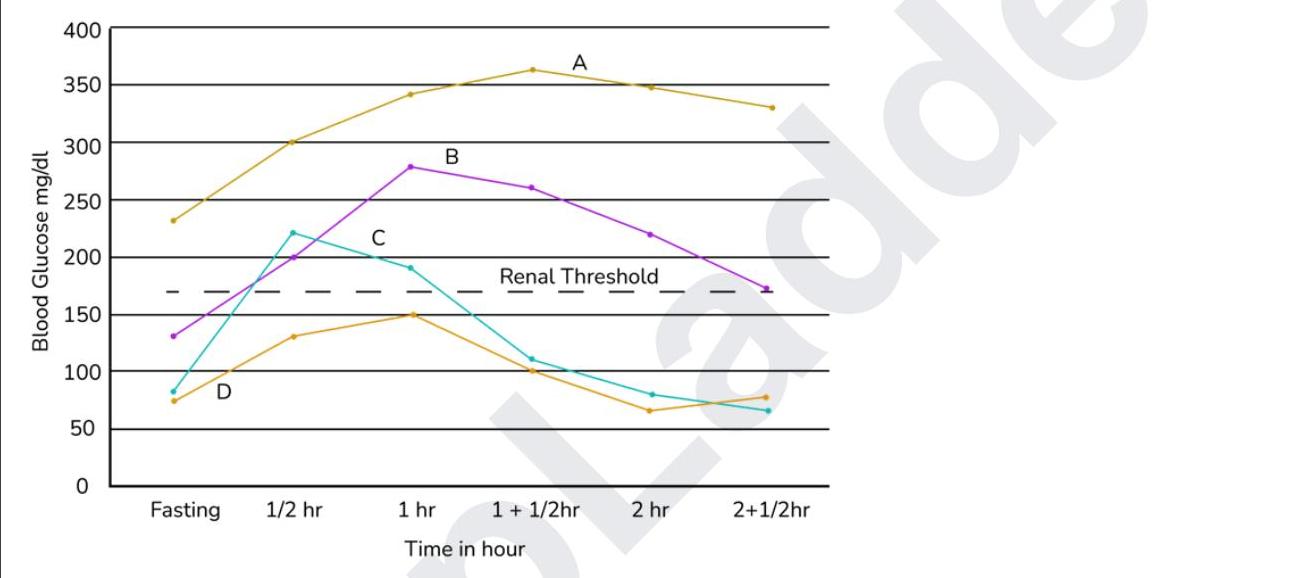
Which of the following represents a normal response to an OGTT?