All (164)Anatomy (15)Anesthesiology (1)Biochemistry (8)Community Medicine (11)Dermatology (7)ENT (2)Forensic Medicine (7)Internal Medicine (16)Microbiology (13)Obstetrics and Gynecology (9)Ophthalmology (3)Orthopaedics (2)Pathology (16)Pediatrics (8)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (12)
Q91
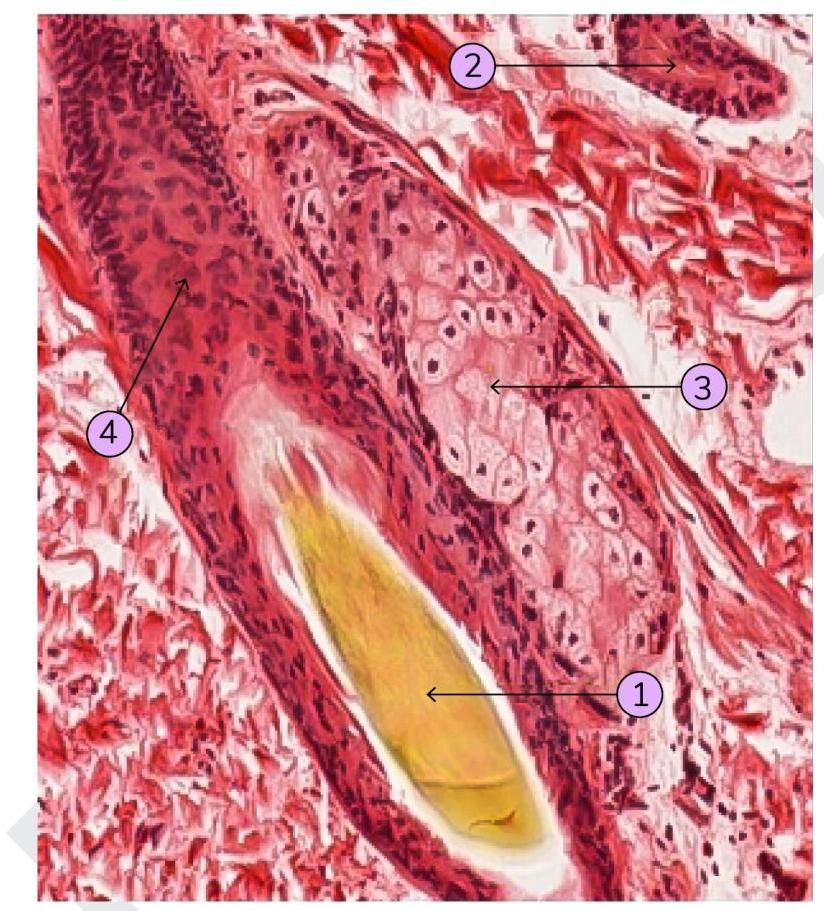
Identify which of the following structure is a sebaceous gland: