INI-CET 2022 — Obstetrics and Gynecology
10 Previous Year Questions with Answers & Explanations
Which of the following is not true about lupus nephritis in pregnancy?
Which of the following is false regarding management of diabetes in pregnancy?
The following cost-effective investigations are routinely recommended in the screening of antenatal mothers, EXCEPT:
Kassowitz rule is related to:
Which hormone is secreted by the placenta?
A 37-year-old unmarried nulliparous woman, having regular intercourse, is on oral contraceptive pills. Her mother was diagnosed with carcinoma breast at 60 years of age, and her elder sister was diagnosed with carcinoma ovary at 40 years of age. What is the next line of management?
The given image depicts:
All of the following can be used in first-trimester medical termination of pregnancy (MTP), except
A woman with eclampsia is started on magnesium sulfate. What is the first sign of magnesium sulfate toxicity?
What is the age group distribution for vulval cancer?
INI-CET 2022 - Obstetrics and Gynecology INI-CET Practice Questions and MCQs
Question 1: Which of the following is not true about lupus nephritis in pregnancy?
- A. Ecosprin, methotrexate, cyclophosphamide, corticosteroids, azathioprine are safe in pregnancy (Correct Answer)
- B. Pregnancy to be planned once the disease has been quiescent for at least 6 months and there is no evidence of renal dysfunction
- C. High dose corticosteroids for lupus flare in pregnancy is safe
- D. Immunosuppression can be continued during pregnancy
Explanation: ***Ecosprin, methotrexate, cyclophosphamide, corticosteroids, azathioprine are safe in pregnancy*** - This statement is **incorrect** because **methotrexate** and **cyclophosphamide** are **contraindicated** in pregnancy due to their teratogenic effects, while **ecosprin (aspirin)** and some **corticosteroids** and **azathioprine** are generally considered relatively safe at appropriate doses. - The combination of **safe and unsafe drugs** within the same statement makes the entire statement untrue; a pregnant patient with lupus nephritis cannot safely take all listed medications. *Pregnancy to be planned once the disease has been quiescent for at least 6 months and there is no evidence of renal dysfunction* - This statement is **true** and represents a **standard recommendation** for managing lupus nephritis in pregnancy. Achieving disease quiescence for at least 6 months significantly reduces the risk of flares and adverse pregnancy outcomes. - Ensuring **absence of renal dysfunction** before conception is crucial to prevent complications like pre-eclampsia, worsening renal function, and prematurity. *High dose corticosteroids for lupus flare in pregnancy is safe* - This statement is **true**. High-dose corticosteroids, such as **prednisone** or **prednisolone**, are often used to manage lupus flares during pregnancy. - These corticosteroids are largely **inactivated by placental enzymes**, minimizing fetal exposure and making them relatively safe for the fetus, while effectively treating maternal disease. *Immunosuppression can be continued during pregnancy* - This statement is **true**. Certain immunosuppressants, like **azathioprine** and **calcineurin inhibitors**, are considered relatively safe and are often continued during pregnancy to prevent disease flares. - **Continuing safe immunosuppression** helps maintain disease control, which is essential for a successful pregnancy outcome in patients with lupus nephritis.
Question 2: Which of the following is false regarding management of diabetes in pregnancy?
- A. In active labor, if RBS <70 mg/dL, D5 is started at 100-150 ml/hr till the RBS is >70 mg/dL
- B. In a patient being planned for induction of labor, night dose of intermediate insulin is given as planned, and the morning dose is withheld
- C. Elective C-section has no role in reducing incidence of brachial plexus injury (Correct Answer)
- D. Capillary blood glucose monitoring levels are kept at fasting- 95 mg/dL; 1 hr postprandial- 140 mg/dL; 2 hrs postprandial- 120 mg/dL
Explanation: ***Elective C-section has no role in reducing incidence of brachial plexus injury*** - This statement is **false** because **elective C-section** can significantly reduce the incidence of **brachial plexus injury** (BPI), especially in cases of suspected fetal macrosomia. - While not universally recommended for all diabetic pregnancies, an elective C-section is considered when the estimated **fetal weight** is substantial or when there's a history of **shoulder dystocia** to prevent birth trauma. *In active labor, if RBS <70 mg/dL, D5 is started at 100-150 ml/hr till the RBS is >70 mg/dL* - This is a **correct** management strategy for **hypoglycemia in labor**. Maintaining stable blood glucose levels (above 70 mg/dL) is crucial to prevent adverse outcomes for both mother and fetus. - The administration of **D5 (dextrose 5% in water)** intravenous solution at a specific rate helps to quickly raise and maintain blood glucose levels. *In a patient being planned for induction of labor, night dose of intermediate insulin is given as planned, and the morning dose is withheld* - This is a common and generally **correct** practice for insulin management before **induction of labor**. The night dose of intermediate insulin helps maintain basal glucose levels overnight. - Withholding the morning dose prevents **hypoglycemia** during labor when food intake is restricted, and insulin sensitivity may increase. Glucose is then typically supplemented through IV fluids as needed. *Capillary blood glucose monitoring levels are kept at fasting- 95 mg/dL; 1 hr postprandial- 140 mg/dL; 2 hrs postprandial- 120 mg/dL* - These are the generally accepted and **correct** target blood glucose levels for **diabetes in pregnancy** (both pre-existing and gestational diabetes). - Achieving these targets is essential to minimize the risk of **fetal macrosomia**, **neonatal hypoglycemia**, and other adverse perinatal outcomes.
Question 3: The following cost-effective investigations are routinely recommended in the screening of antenatal mothers, EXCEPT:
- A. Blood sugar levels for GDM
- B. VDRL for syphilis
- C. Urine analysis for bacteriuria
- D. Echocardiography for cardiac disease (Correct Answer)
Explanation: ***Echocardiography for cardiac disease*** - **Echocardiography** is not a *routinely recommended* screening investigation for all antenatal mothers due to its cost and the relatively low prevalence of significant congenital heart disease requiring universal screening. - It is typically performed only if there are **specific risk factors** or suspicious findings suggesting cardiac pathology. *Blood sugar levels for GDM* - Screening for **gestational diabetes mellitus (GDM)** with blood sugar levels (e.g., glucose challenge test) is routinely recommended due to the potential maternal and fetal complications if untreated. - GDM is a common condition that can be effectively managed with early diagnosis, making screening a **cost-effective** preventive measure. *VDRL for syphilis* - Screening for **syphilis** using tests like VDRL (Venereal Disease Research Laboratory) is a standard and *routinely recommended* antenatal investigation. - Early detection and treatment of syphilis in pregnant women prevent serious adverse outcomes such as **congenital syphilis**, which can cause severe fetal morbidity and mortality. *Urine analysis for bacteriuria* - **Urine analysis** for **asymptomatic bacteriuria** is routinely recommended during pregnancy because untreated bacteriuria can lead to pyelonephritis, preterm labor, and low birth weight. - It is a simple, **cost-effective** test with significant benefits for maternal and fetal health.
Question 4: Kassowitz rule is related to:
- A. Congenital syphilis (Correct Answer)
- B. Primary syphilis
- C. Latent syphilis
- D. Secondary syphilis
Explanation: ***Congenital syphilis*** - The **Kassowitz rule** specifically describes the high rate of perinatal mortality (abortion, stillbirth, or death shortly after birth) in cases of untreated maternal syphilis, especially during early stages of infection. - It highlights that the risk is highest when the mother acquires syphilis shortly before or during pregnancy, leading to severe fetal disease. *Primary syphilis* - This stage is characterized by a **chancre** at the site of infection and is the initial presentation in the infected individual, not directly related to fetal outcomes. - While primary syphilis in the mother can lead to congenital syphilis, the Kassowitz rule itself describes the outcome of congenital infection, not the primary infection in the mother. *Latent syphilis* - **Latent syphilis** refers to a stage where the infection is present but asymptomatic, potentially for years. - While it can be transmitted vertically and lead to congenital syphilis, the Kassowitz rule specifically quantifies the mortality risk of congenital syphilis, not the mother's latent infection itself. *Secondary syphilis* - This stage involves a systemic rash and other widespread symptoms in the infected individual, appearing weeks to months after the chancre. - Though highly infectious and a significant risk for vertical transmission, the rule focuses on the severe consequences *for the fetus* when congenital syphilis occurs, not the symptoms of secondary syphilis in the mother.
Question 5: Which hormone is secreted by the placenta?
- A. GnRH
- B. FSH
- C. hCG (Correct Answer)
- D. LH
Explanation: ***hCG*** - **Human Chorionic Gonadotropin (hCG)** is produced by the **syncytiotrophoblast** of the placenta shortly after implantation. - Its primary role is to maintain the **corpus luteum**, ensuring continued production of **progesterone** to support the pregnancy. *GnRH* - **Gonadotropin-releasing hormone (GnRH)** is secreted by the **hypothalamus** in the brain, not the placenta. - It stimulates the pituitary gland to release FSH and LH. *FSH* - **Follicle-stimulating hormone (FSH)** is produced by the **anterior pituitary gland**. - It plays a crucial role in ovarian follicular development in females and spermatogenesis in males. *LH* - **Luteinizing hormone (LH)** is also secreted by the **anterior pituitary gland**. - Its functions include triggering ovulation in females and stimulating testosterone production in males.
Question 6: A 37-year-old unmarried nulliparous woman, having regular intercourse, is on oral contraceptive pills. Her mother was diagnosed with carcinoma breast at 60 years of age, and her elder sister was diagnosed with carcinoma ovary at 40 years of age. What is the next line of management?
- A. Prophylactic surgery
- B. Stop taking oral contraceptive pills
- C. Routine mammography
- D. Genetic counseling and screening for BRCA (Correct Answer)
Explanation: ***Genetic counseling and screening for BRCA*** - The patient's family history is highly suggestive of a **hereditary breast and ovarian cancer (HBOC) syndrome**, specifically a BRCA gene mutation. - **Sister with ovarian cancer at age 40** is a major red flag—ovarian cancer at ≤50 years in a first-degree relative is a specific criterion for BRCA testing according to NCCN guidelines. - Additionally, the mother's breast cancer (even at 60) combined with the sister's early ovarian cancer creates a **two first-degree relatives with breast/ovarian cancer pattern** that further strengthens the indication for genetic testing. - **Genetic counseling** is essential to assess risk, discuss testing options, interpret results, and plan appropriate risk-reduction strategies. - BRCA1/2 mutations confer a **40-60% lifetime risk of ovarian cancer** and **70-80% lifetime risk of breast cancer**. *Prophylactic surgery* - **Risk-reducing bilateral salpingo-oophorectomy (RRSO)** and possibly bilateral mastectomy are important options for BRCA mutation carriers, but should only be considered **after** genetic counseling and confirmed identification of a pathogenic mutation. - Proceeding directly to surgery without genetic confirmation would be premature and potentially unnecessary. *Stop taking oral contraceptive pills* - **OCPs actually reduce ovarian cancer risk** by approximately 50% with long-term use, which is protective even in BRCA carriers. - While OCPs may have a minimal impact on breast cancer risk, the ovarian cancer risk reduction benefit generally outweighs this concern. - Stopping OCPs without further genetic risk assessment is not the appropriate next step. *Routine mammography* - Standard mammography screening is insufficient for high-risk individuals with likely BRCA mutations. - If BRCA mutation is confirmed, enhanced screening protocols are recommended: **annual MRI plus mammography starting at age 30**, or 10 years before the earliest breast cancer in the family. - The priority is genetic assessment first to determine if intensified screening is warranted.
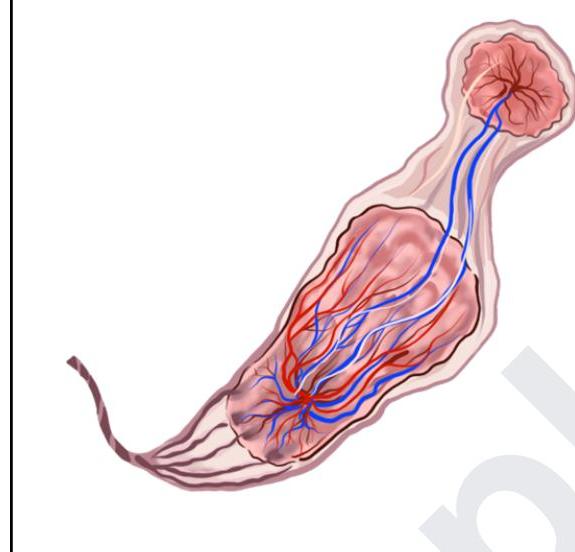
Question 7: The given image depicts:
- A. Normal placenta
- B. Succenturiate lobe
- C. Both succenturiate lobe and velamentous insertion (Correct Answer)
- D. Velamentous insertion of the cord
Explanation: ***Both succenturiate lobe and velamentous insertion*** - The image clearly depicts two distinct placental lobes (**succenturiate lobes**), with a smaller accessory lobe separate from the main placental body. - The **umbilical vessels** are also seen running through the fetal membranes before reaching the placental tissue, which is characteristic of **velamentous insertion**. *Normal placenta* - A normal placenta consists of a **single, unified organ** directly attached to the decidua, with the umbilical cord inserting centrally or eccentrically into this main mass. - The **umbilical cord** in a normal placenta would insert directly into the placental tissue, not into the membranes. *Succenturiate lobe* - A succenturiate lobe (or accessory lobe) refers to one or more small lobes of the placenta located at a distance from the main placental body. - While a succenturiate lobe is present, the image also shows the umbilical vessels traversing the membranes, indicating an additional anomaly known as **velamentous insertion**, making this option incomplete. *Velamentous insertion of the cord* - Velamentous insertion is characterized by the **umbilical blood vessels** separating before reaching the placental disc, traveling through the fetal membranes. - While velamentous insertion is evident, the presence of a **separate accessory lobe** makes this option incomplete as it doesn't account for both depicted abnormalities.
Question 8: All of the following can be used in first-trimester medical termination of pregnancy (MTP), except
- A. Manual vacuum aspiration
- B. Dilatation and curettage
- C. Extra-amniotic instillation of ethacridine lactate (Correct Answer)
- D. Mifepristone + misoprostol
Explanation: ***Extra-amniotic instillation of ethacridine lactate*** - **Extra-amniotic instillation of ethacridine lactate** is a method primarily used for **second-trimester** pregnancy terminations. - Its mechanism involves causing inflammation and contraction of the uterus, which is less effective and carries higher risks in the first trimester. *Manual vacuum aspiration* - **Manual vacuum aspiration (MVA)** is a common and effective surgical method for **first-trimester MTP**. - It involves using a syringe and cannula to remove the uterine contents directly. *Dilatation and curettage* - **Dilatation and curettage (D&C)** is another standard surgical procedure used for **first-trimester MTP**. - It involves dilating the cervix and using a curette to scrape the uterine lining and remove the pregnancy tissue. *Mifepristone + misoprostol* - The combination of **mifepristone and misoprostol** is the most common and effective medical method for **first-trimester MTP**. - **Mifepristone** blocks progesterone, while **misoprostol** causes uterine contractions and cervical ripening, expelling the pregnancy.
Question 9: A woman with eclampsia is started on magnesium sulfate. What is the first sign of magnesium sulfate toxicity?
- A. Respiratory depression
- B. Hypotension
- C. Loss of knee jerk (Correct Answer)
- D. Reduced muscle tone
Explanation: ***Loss of knee jerk*** - **Diminished or absent deep tendon reflexes**, particularly the knee jerk, is the **earliest clinical sign** of magnesium sulfate toxicity. - This occurs at serum magnesium levels between **7-10 mEq/L** (8.5-12 mg/dL) due to magnesium's depressant effect on the nervous system and neuromuscular transmission. *Respiratory depression* - **Respiratory depression** is a more severe and later sign of magnesium toxicity, occurring at higher serum levels (typically >12 mEq/L). - It indicates significant central nervous system depression and potential for respiratory arrest, usually after reflexes are already lost. *Hypotension* - While magnesium sulfate can cause **vasodilation** and a subsequent drop in blood pressure, it is generally **not the first sign of toxicity** and often occurs concurrently with other mild to moderate signs. - Hypotension may be part of the therapeutic effect to reduce blood pressure in eclampsia, rather than an initial indicator of toxicity. *Reduced muscle tone* - **Reduced muscle tone** or **flaccidity** is also a consequence of magnesium's neuromuscular blocking effect but typically manifests **after the loss of deep tendon reflexes**. - It signifies more profound neuromuscular impairment, closer to the progression towards respiratory depression.
Question 10: What is the age group distribution for vulval cancer?
- A. 65-85 years
- B. 35-55 years
- C. Not age specific
- D. Both age groups (35-55 and 65-85 years) (Correct Answer)
Explanation: ***Both age groups (35-55 and 65-85 years)*** - Vulval cancer demonstrates a **bimodal age distribution**, meaning it presents with two distinct peaks of incidence. - The first peak occurs in younger women, typically aged **35-55 years**, often associated with **HPV infection** and vulvar intraepithelial neoplasia (VIN). - The second peak is seen in older women, aged **65-85 years**, where the disease is more commonly linked to **chronic inflammatory conditions** such as lichen sclerosus, often without HPV involvement. - This bimodal pattern reflects the **two distinct pathogenic pathways** of vulval cancer: HPV-related and non-HPV-related disease. *65-85 years* - While this age group represents a significant peak of vulval cancer incidence, particularly in cases **unrelated to HPV**, it does not encompass the entire distribution. - Focusing solely on this age range would **miss cases occurring in younger women**, which are increasingly recognized due to HPV-related disease. *35-55 years* - This age group does indeed represent a distinct peak for vulval cancer, especially in cases linked to **Human Papillomavirus (HPV) infection**. - However, ignoring the incidence in older women would provide an **incomplete understanding** of the disease's overall epidemiology. *Not age specific* - Vulval cancer is definitely **age-specific** with distinct age group distributions. - The incidence is **not uniformly distributed** across all ages but rather shows an increased likelihood within specific age ranges, demonstrating clear bimodal peaks.