INI-CET 2022 — Internal Medicine
18 Previous Year Questions with Answers & Explanations
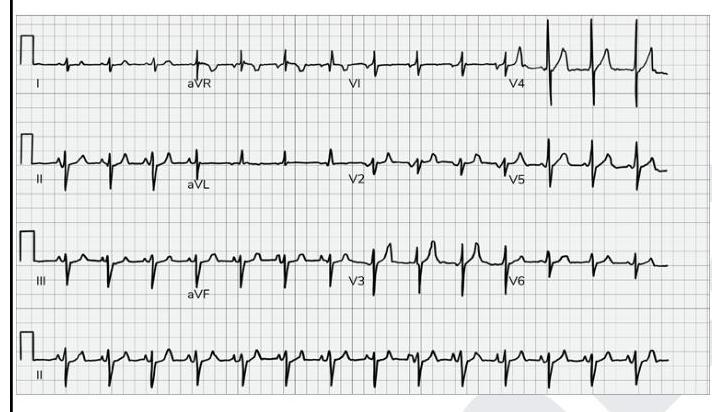
What does the given ECG show?
Which of the following statements are true about familial adenomatous polyposis? 1. It is autosomal recessive 2. If not treated, 100% of the cases progress to adenocarcinoma colon. 3. It is associated with a gene mutation in KRAS 4. It is associated with congenital hypertrophy of the retinal pigment epithelium.
A patient presented with reduced levels of high-density lipoprotein, and ABCA1 mutation. On examination, tonsils appeared as shown in the image. What is the diagnosis?

A diabetic patient's fasting blood glucose level is found to be $160 \mathrm{mg} / \mathrm{dL}$. What will you advise the patient regarding non-pharmacological management?
Which of the following is not a first-line drug for the management of a patient with rheumatoid arthritis?
The following are parvovirus - related disease - population pairs. Identify the incorrect pair. 1. Aplastic anemia - Patient with hereditary hemolytic anemia 2. Non - immune hydrops - pregnant women 3. Erythema infectiosum - infants 4. Non - erosive arthritis - Patients of SLE
Mark the correct statement regarding inflammatory bowel disease.
A person presents to the hospital with fever and chills. Fever profile is ordered and is found to be negative for malaria and dengue. Rk39 test is found to be positive. What is the treatment of choice?
Incorrect statement regarding the management of frostbite:
A patient, who is a known case of HIV with a CD4 count of 200 cells/cu.mm, presents with 5 days of cough and high-grade fever without chills and rigors. There is no history of diarrhoea, vomiting, or nuchal rigidity. Chest x-ray is normal. What treatment will you give?
INI-CET 2022 - Internal Medicine INI-CET Practice Questions and MCQs
Question 1: What does the given ECG show?
- A. P-pulmonale (Correct Answer)
- B. Improper calibration
- C. Electrical alternans
- D. Ventricular bigeminy
Explanation: ***P-pulmonale*** - The ECG shows tall, peaked **P waves** with an amplitude of more than **2.5 mm in lead II**, which is characteristic of P-pulmonale. - P-pulmonale indicates **right atrial enlargement or hypertrophy**, often due to conditions like severe lung disease (e.g., COPD) or pulmonary hypertension. *Improper calibration* - Improper calibration would typically affect the amplitude of all ECG complexes globally or specific leads consistently, which is not the primary finding here. - The calibration mark (first beat in lead I) appears normal, indicating standard calibration (10mm/mV). *Electrical alternans* - **Electrical alternans** is characterized by beat-to-beat variation in the QRS complex amplitude, which is not visible in this ECG. - It is commonly associated with **pericardial effusion with cardiac tamponade**. *Ventricular bigeminy* - **Ventricular bigeminy** is a pattern where every normal sinus beat is followed by a premature ventricular contraction (PVC). - This ECG shows a regular rhythm with consistent P-QRS-T morphology, without alternating normal and PVC beats.
Question 2: Which of the following statements are true about familial adenomatous polyposis? 1. It is autosomal recessive 2. If not treated, 100% of the cases progress to adenocarcinoma colon. 3. It is associated with a gene mutation in KRAS 4. It is associated with congenital hypertrophy of the retinal pigment epithelium.
- A. 2 and 4 (Correct Answer)
- B. None of the options
- C. 1 and 4
- D. 2 and 3
Explanation: ***2 and 4*** - Without treatment, **familial adenomatous polyposis (FAP)** leads to colorectal **adenocarcinoma** in 100% of cases, due to the accumulation of numerous adenomatous polyps throughout the colon. - FAP is strongly associated with **congenital hypertrophy of the retinal pigment epithelium (CHRPE)**, which can be an early diagnostic marker [1]. *None of the options* - This statement is incorrect because FAP does indeed involve the progression to adenocarcinoma and is associated with CHRPE. - The combination of these two true statements makes this option invalid. *1 and 4* - FAP is inherited in an **autosomal dominant** manner, not autosomal recessive [1]. - While statement 4 (association with CHRPE) is true, statement 1 being false makes this option incorrect. *2 and 3* - Although statement 2 (100% progression to adenocarcinoma) is true, statement 3 is incorrect. - FAP is primarily caused by mutations in the **APC gene**, not the KRAS gene [1]. KRAS is more commonly associated with sporadic colorectal cancer progression rather than FAP.
Question 3: A patient presented with reduced levels of high-density lipoprotein, and ABCA1 mutation. On examination, tonsils appeared as shown in the image. What is the diagnosis?
- A. Tangier disease (Correct Answer)
- B. Fabry disease
- C. Niemann-Pick disease
- D. Gaucher disease
Explanation: ***Tangier disease*** - This condition is characterized by **very low HDL levels** due to mutations in the **ABCA1 gene**, which impairs cholesterol efflux from cells. - The classic physical finding is **enlarged, orange-yellow tonsils** due to cholesterol ester deposition, seen in the provided image. *Fabry disease* - This is an **X-linked lysosomal storage disorder** caused by a deficiency of **alpha-galactosidase A**, leading to globotriaosylceramide accumulation. - Clinical features include **neuropathic pain**, **angiokeratomas**, **corneal opacities**, and early renal and cardiac disease, not orange-yellow tonsils. *Niemann-Pick disease* - This is a group of **autosomal recessive lysosomal storage disorders** caused by deficiencies in enzymes like acid sphingomyelinase or proteins involved in cholesterol processing. - It typically presents with **hepatosplenomegaly**, **neurodegeneration** (especially type A and B), and **lung involvement**, but not oral lesions as depicted. *Gaucher disease* - This is an **autosomal recessive lysosomal storage disease** resulting from a deficiency of the enzyme **beta-glucosidase**, leading to accumulation of glucocerebroside. - Characteristic features include **hepatosplenomegaly**, **bone pain** and crises, and **pancytopenia**, without any specific tonsillar findings.
Question 4: A diabetic patient's fasting blood glucose level is found to be $160 \mathrm{mg} / \mathrm{dL}$. What will you advise the patient regarding non-pharmacological management?
- A. At least 25-35 g of dietary fibre
- B. <30 % of the calories should come from fat (Correct Answer)
- C. Dietary cholesterol <300 mg per day
- D. <2.3 g sodium intake every day
Explanation: ***<30 % of the calories should come from fat*** - Reducing dietary fat intake to less than 30% of total calories is a crucial non-pharmacological strategy for diabetic patients to manage blood glucose levels and prevent cardiovascular complications [1]. - Excess dietary fat, especially saturated and trans fats, can contribute to insulin resistance and weight gain, both of which negatively impact glycemic control [1]. *At least 25-35 g of dietary fibre* - While adequate dietary fiber (typically 25-30g for adults, sometimes up to 35g for men) is beneficial for managing blood glucose, it is generally recommended as a baseline for healthy eating and not the primary or most impactful intervention to address a fasting glucose of 160 mg/dL [1]. - Fiber helps slow glucose absorption and can improve insulin sensitivity, but a specific "at least 25-35g" statement without further context on total caloric intake or other macronutrient distribution might not be the most targeted advice for this specific glucose level [1]. *Dietary cholesterol <300 mg per day* - Limiting dietary cholesterol to less than 300 mg per day is a general recommendation for cardiovascular health, which is particularly important for diabetic patients due to their increased risk of atherosclerosis [2]. - However, for directly addressing a fasting blood glucose of 160 mg/dL, focusing on overall fat intake and carbohydrate quality would have a more immediate impact on glucose control than dietary cholesterol alone. *<2.3 g sodium intake every day* - Restricting sodium intake to less than 2.3 g per day is recommended for managing hypertension and reducing cardiovascular risk, which is often comorbid with diabetes [2]. - While important for overall health in diabetic patients, this recommendation does not directly target blood glucose control and would not be the primary non-pharmacological advice for a fasting glucose of 160 mg/dL.
Question 5: Which of the following is not a first-line drug for the management of a patient with rheumatoid arthritis?
- A. Hydroxychloroquine
- B. Sulfasalazine
- C. Azathioprine (Correct Answer)
- D. Methotrexate
Explanation: ***Azathioprine*** - While an **immunosuppressant**, azathioprine is generally reserved for patients with **refractory rheumatoid arthritis (RA)** or those who cannot tolerate or have failed first-line DMARDs. - Its use often comes with a higher risk of side effects, making it less suitable as an initial agent compared to other conventional synthetic DMARDs. *Hydroxychloroquine* - This is a **first-line DMARD** for RA, particularly in patients with **mild disease**, due to its relatively favorable safety profile. - It is often used in combination with other DMARDs like methotrexate. *Sulfasalazine* - Sulfasalazine is a common **first-line conventional synthetic DMARD** for RA, especially effective in patients with peripheral arthritis. - It is frequently used when methotrexate is contraindicated or not tolerated, or as part of combination therapy. *Methotrexate* - **Methotrexate is considered the cornerstone** and **first-line treatment** for most patients with rheumatoid arthritis due to its efficacy and tolerability [1]. - It is recommended for early initiation in newly diagnosed patients to prevent joint damage and improve outcomes [2].
Question 6: The following are parvovirus - related disease - population pairs. Identify the incorrect pair. 1. Aplastic anemia - Patient with hereditary hemolytic anemia 2. Non - immune hydrops - pregnant women 3. Erythema infectiosum - infants 4. Non - erosive arthritis - Patients of SLE
- A. 1
- B. 2
- C. 3
- D. 4 (Correct Answer)
Explanation: ***Non - erosive arthritis - Patients of SLE*** - While parvovirus B19 can cause **non-erosive arthritis**, it is not specifically associated with patients with **systemic lupus erythematosus (SLE)** as a common or unique presentation. Parvovirus B19-induced arthritis typically resolves spontaneously. [1] - The given pairing implies a direct and specific link between parvovirus B19 arthritis and SLE patients, which is inaccurate. *Aplastic anemia - Patient with hereditary hemolytic anemia* - This is a **correct pairing**. Parvovirus B19 preferentially infects and destroys erythroid progenitor cells, leading to a temporary cessation of red blood cell production. [1] - In patients with **hereditary hemolytic anemias** (e.g., sickle cell anemia, thalassemia), who have a rapid red blood cell turnover and depend on continuous erythropoiesis, this cessation can lead to a severe and life-threatening **aplastic crisis**. [1] *Non - immune hydrops - pregnant women* - This is a **correct pairing**. Parvovirus B19 infection in a pregnant woman can cross the placenta and infect the fetus. - Fetal infection can cause severe anemia and heart failure, leading to **non-immune hydrops fetalis**, a condition characterized by abnormal fluid accumulation in two or more fetal compartments. *Erythema infectiosum - infants* - This is a **correct pairing**. **Erythema infectiosum**, also known as "fifth disease," is the most common clinical manifestation of parvovirus B19 infection. [1] - It primarily affects **children** (including infants) and is characterized by a "slapped cheek" rash on the face followed by a lacy rash on the trunk and extremities. [1]
Question 7: Mark the correct statement regarding inflammatory bowel disease.
- A. Skip lesions are present in Crohn's disease (Correct Answer)
- B. Inflammatory bowel disease doesn't have a genetic predisposition
- C. Crohn's is curable through surgical resection of the affected segment
- D. Mucosal layers are involved in Crohn's while transmural involvement seen in ulcerative colitis
Explanation: ***Skip lesions are present in Crohn's disease*** - **Skip lesions** refer to the characteristic patchy, discontinuous areas of inflammation seen in **Crohn's disease**, where affected segments of the bowel are separated by healthy areas. - This feature is a key differentiator from ulcerative colitis, which typically exhibits **continuous inflammation**. *Inflammatory bowel disease doesn't have a genetic predisposition* - **Genetic predisposition** plays a significant role in both Crohn's disease and ulcerative colitis, with multiple genes identified that increase susceptibility. - A family history of IBD is a well-established risk factor, indicating its genetic component. *Crohn's is curable through surgical resection of the affected segment* - Crohn's disease is a **chronic, relapsing condition** that can affect any part of the gastrointestinal tract, and while surgery can remove affected segments, it is not curative. - Disease often **recurs in other parts** of the GI tract even after surgical resection. *Mucosal layers are involved in Crohn's while transmural involvement seen in ulcerative colitis* - This statement is incorrect; **Crohn's disease** is characterized by **transmural inflammation** (involving all layers of the bowel wall). - **Ulcerative colitis** primarily affects the **mucosal and submucosal layers** of the large intestine.
Question 8: A person presents to the hospital with fever and chills. Fever profile is ordered and is found to be negative for malaria and dengue. Rk39 test is found to be positive. What is the treatment of choice?
- A. Amphotericin B (Correct Answer)
- B. Dapsone
- C. Hydroxychloroquine
- D. Griseofulvin
Explanation: Amphotericin B - A positive RK39 test suggests visceral leishmaniasis (kala-azar), especially with fever and chills in an endemic area [1]. - Amphotericin B (specifically liposomal Amphotericin B) is a highly effective and often the drug of choice for treating visceral leishmaniasis, particularly in severe cases or regions with antimonial resistance. Dapsone - Dapsone is primarily used in the treatment of leprosy and بعض forms of dermatitis (e.g., dermatitis herpetiformis). - It has no significant role in treating leishmaniasis. Hydroxychloroquine - Hydroxychloroquine is an antimalarial drug also used for certain autoimmune diseases like lupus and rheumatoid arthritis [2]. - It is ineffective against leishmaniasis. Griseofulvin - Griseofulvin is an antifungal medication used to treat dermatophyte infections (e.g., ringworm of the skin, hair, or nails). - It has no activity against Leishmania parasites.
Question 9: Incorrect statement regarding the management of frostbite:
- A. Antibiotics and analgesics not used (Correct Answer)
- B. Amputation in severe cases
- C. Rewarming is done
- D. The area is dried and cleaned
Explanation: ***Antibiotics and analgesics not used*** - This statement is incorrect as **antibiotics are used** in the management of frostbite for prophylaxis against infection, especially in severe cases or open wounds. - **Analgesics are also crucial** to manage the significant pain associated with frostbite and the rewarming process [1]. *Amputation in severe cases* - **Amputation** is a necessary intervention for severe, irreversible tissue damage and necrosis caused by frostbite, typically reserved as a last resort [1]. - This decision is usually made after sufficient time has passed to demarcate viable from non-viable tissue, often several weeks post-injury [1]. *Rewarming is done* - **Rapid rewarming** of the affected area in a warm water bath (37-39°C) is the most critical initial treatment for frostbite to minimize tissue damage. - This process is painful and should be done only when there is no risk of refreezing. *The area is dried and cleaned* - After rewarming, the affected area should be **gently dried** to prevent further skin breakdown and the development of maceration. - **Cleaning the wound** helps prevent infection and maintains a sterile environment for healing.
Question 10: A patient, who is a known case of HIV with a CD4 count of 200 cells/cu.mm, presents with 5 days of cough and high-grade fever without chills and rigors. There is no history of diarrhoea, vomiting, or nuchal rigidity. Chest x-ray is normal. What treatment will you give?
- A. Co-trimoxazole + steroids
- B. Co-trimoxazole only (Correct Answer)
- C. Amoxicillin-clavulanic acid + Azithromycin
- D. Antitubercular treatment
Explanation: ***Co-trimoxazole only*** - The patient has a CD4 count of 200 cells/cu.mm with cough and fever and a normal chest X-ray, all of which are highly suggestive of **Pneumocystis jirovecii pneumonia (PJP)**, even without classic infiltrates. Therefore, **co-trimoxazole** (trimethoprim-sulfamethoxazole) is the first-line treatment [1]. - In a patient with HIV and a CD4 count below 200, **PJP prophylaxis** with co-trimoxazole should also be considered [2], and its empirical treatment is indicated in this scenario. *Co-trimoxazole + steroids* - While co-trimoxazole is the correct treatment for PJP, **steroids** are typically reserved for patients with more severe disease, indicated by **hypoxia** (PaO2 < 70 mmHg or A-a gradient > 35 mmHg) or diffuse interstitial infiltrates on chest imaging, neither of which are described here [1]. - Adding steroids without clear indications could increase the risk of side effects in an immunocompromised patient. *Amoxicillin-clavulanic acid + Azithromycin* - This combination targets typical **bacterial community-acquired pneumonia**, which is less likely given the patient's HIV status, low CD4 count, and normal chest X-ray. - This regimen would not effectively treat **PJP**, which is the most probable diagnosis in this immunocompromised setting. *Antitubercular treatment* - While tuberculosis is common in HIV patients, the normal chest X-ray makes pulmonary tuberculosis less likely, especially without other classic symptoms like night sweats, weight loss, or hemoptysis. In patients with CD4 counts below 200, the clinical presentation of TB differences substantially from those without HIV [1]. - **Antitubercular treatment** would not address the immediate concern of possible PJP, which can rapidly progress if untreated.