A 12-week pregnant woman on multidrug therapy for leprosy presents with type 2 lepra reaction. What is the treatment of choice for this patient?
Q2
Match the following scale types with their lesions.
| Scales | Lesions |
| :-- | :-- |
| 1. Collarette scales | a. Pityriasis versicolour |
| 2. Silvery scales | b. Pityriasis rosea |
| 3. Mica-like scales | c. Psoriasis |
| 4. Branny scales | d. Pityriasis lichenoides |
Q3
A 60-year-old patient presents with unilateral vesicular lesions in a dermatomal distribution on the torso. The lesions are painful and appeared over the past 2-3 days, progressing from erythematous patches to fluid-filled vesicles. The patient reports prodromal burning and tingling sensation in the affected area. Which of the following is the most likely diagnosis?
Q4
Consider the following causes of alopecia: 1. Androgenetic alopecia 2. Alopecia areata 3. Telogen effluvium 4. Lichen planopilaris. Which among the following causes non-scarring alopecia?
Q5
A woman presents with lesions on the inner thighs and peri-anal region. They are nodular, 4-6 mm in size and appear pale. The histopathological image shows multiple intracytoplasmic inclusion bodies consistent with Henderson-Patterson bodies. The diagnosis is:
Q6
A 7-year-old child presents to the dermatology clinic with multiple small, painless, flesh-colored papules on the trunk and arms that have been present for 3 months. The lesions are 2-4 mm in diameter, dome-shaped with a smooth surface, and several have a characteristic central umbilication. The child is otherwise healthy and immunocompetent. The lesions are not pruritic and there is no associated lymphadenopathy. On closer examination, a white, cheesy material can be expressed from the central depression of some lesions.
What is the most likely diagnosis?
INI-CET 2022 - Dermatology INI-CET Practice Questions and MCQs
Question 1: A 12-week pregnant woman on multidrug therapy for leprosy presents with type 2 lepra reaction. What is the treatment of choice for this patient?
A. Continue MDT and add oral steroids (Correct Answer)
B. Antibiotics
C. Stop MDT and start oral steroids
D. Thalidomide
Explanation: ***Continue MDT and add oral steroids***
- **Type 2 lepra reactions (erythema nodosum leprosum)** are inflammatory complications of leprosy and require systemic anti-inflammatory treatment. **Oral corticosteroids** are the mainstay for managing these reactions, particularly in pregnant patients where other immunomodulators are contraindicated.
- **Multidrug therapy (MDT)** for leprosy should be continued throughout the reaction, even during pregnancy, to ensure eradication of <b>*Mycobacterium leprae*</b> and prevent drug resistance. Interrupting MDT can lead to relapse and increased neurological damage.
*Antibiotics*
- This option is incorrect because the type 2 lepra reaction is an **immunological complication** of leprosy, not a bacterial infection requiring additional antibiotics beyond the standard MDT.
- The symptoms are due to the immune system's response to dying bacteria, not a new or secondary bacterial infection.
*Stop MDT and start oral steroids*
- Stopping MDT is inappropriate as the underlying **leprosy infection** still needs to be treated to prevent further progression and drug resistance.
- While steroids are crucial for managing the reaction, stopping MDT would compromise the **curative treatment** for leprosy.
*Thalidomide*
- **Thalidomide** is highly effective in treating **erythema nodosum leprosum (ENL)**.
- However, it is an absolute **contraindication** during pregnancy due to its severe **teratogenicity**, causing severe birth defects.
Question 2: Match the following scale types with their lesions.
| Scales | Lesions |
| :-- | :-- |
| 1. Collarette scales | a. Pityriasis versicolour |
| 2. Silvery scales | b. Pityriasis rosea |
| 3. Mica-like scales | c. Psoriasis |
| 4. Branny scales | d. Pityriasis lichenoides |
A. 1-d, 2-c, 3-a, 4-b
B. 1-c, 2-b, 3-d, 4-a
C. 1-a, 2-b, 3-d, 4-c
D. 1-b, 2-c, 3-d, 4-a (Correct Answer)
Explanation: ***1-b, 2-c, 3-d, 4-a***
- **Collarette scales** are pathognomonic of **Pityriasis rosea**, appearing as fine, trailing scales around the periphery of oval lesions in a "Christmas tree" distribution.
- **Silvery scales** are the classic hallmark of **Psoriasis**, presenting as thick, adherent, silvery-white scales overlying well-demarcated erythematous plaques.
- **Mica-like scales** are characteristic of **Pityriasis lichenoides**, appearing as thick, shiny, adherent scales that can be peeled off like mica sheets.
- **Branny scales** are typical of **Pityriasis versicolor**, presenting as fine, powdery scales caused by **Malassezia** yeast overgrowth.
*1-d, 2-c, 3-a, 4-b*
- Incorrectly matches **collarette scales with Pityriasis lichenoides**, which typically presents with mica-like scales, not collarette scales.
- Misassociates **mica-like scales with Pityriasis versicolor**, which characteristically has branny (fine, powdery) scales.
*1-c, 2-b, 3-d, 4-a*
- Wrongly pairs **collarette scales with Psoriasis**, which is known for thick silvery scales, not peripheral collarette scales.
- Incorrectly matches **silvery scales with Pityriasis rosea**, which has collarette scales at lesion periphery, not silvery scales.
*1-a, 2-b, 3-d, 4-c*
- Falsely associates **collarette scales with Pityriasis versicolor**, which has branny scales from yeast infection, not collarette scales.
- Mismatches **branny scales with Psoriasis**, which has characteristic thick silvery scales, not fine powdery scales.
Question 3: A 60-year-old patient presents with unilateral vesicular lesions in a dermatomal distribution on the torso. The lesions are painful and appeared over the past 2-3 days, progressing from erythematous patches to fluid-filled vesicles. The patient reports prodromal burning and tingling sensation in the affected area. Which of the following is the most likely diagnosis?
A. Herpes zoster infection (Correct Answer)
B. Irritant contact dermatitis
C. Allergic contact dermatitis
D. Herpes Simplex Infection
Explanation: ***Herpes zoster infection***
- The patient's presentation of **unilateral vesicular lesions** in a **dermatomal distribution**, accompanied by severe pain and a **prodromal burning and tingling sensation**, is classic for herpes zoster (shingles).
- Herpes zoster results from the **reactivation of latent varicella-zoster virus (VZV)** in a sensory ganglion, leading to painful rash along the affected nerve path.
*Irritant contact dermatitis*
- This condition involves inflammation due to direct contact with an irritating substance, often presenting with **eczematous lesions**, redness, itching, and sometimes vesicles.
- However, it typically lacks the characteristic **dermatomal distribution** and severe neuropathic pain seen in herpes zoster.
*Allergic contact dermatitis*
- Allergic contact dermatitis is an immune-mediated reaction to an allergen, causing intensely pruritic, erythematous, and often **vesicular or bullous eruptions** that tend to spread beyond the initial contact area over time.
- While it can cause vesicles, it does not follow a **dermatomal pattern** and is usually very itchy, rather than primarily painful and burning, with a distinct prodrome.
*Herpes Simplex Infection*
- Herpes simplex virus (HSV) infections also cause **vesicular lesions** but typically present as clusters of vesicles on an **erythematous base** in a localized area, often around the mouth (cold sores) or genitals.
- Unlike herpes zoster, HSV lesions are usually **recurrent** in the same small area and typically do not exhibit a widespread, **unilateral dermatomal pattern** or the associated severe, persistent neuropathic pain.
Question 4: Consider the following causes of alopecia: 1. Androgenetic alopecia 2. Alopecia areata 3. Telogen effluvium 4. Lichen planopilaris. Which among the following causes non-scarring alopecia?
A. 1, 2 and 3 (Correct Answer)
B. Only 4
C. 3 and 4
D. 2, 3 and 4
Explanation: **1, 2, and 3**
- **Androgenetic alopecia**, **alopecia areata**, and **telogen effluvium** are all forms of **non-scarring alopecia**, meaning the hair follicles are primarily affected without permanent destruction.
- In these conditions, there is potential for hair regrowth as the follicular structures remain intact.
*Only 4*
- **Lichen planopilaris** is a type of **scarring alopecia**, characterized by permanent destruction of hair follicles and replacement with fibrous tissue.
- This leads to irreversible hair loss in the affected areas.
*3 and 4*
- While **telogen effluvium** causes non-scarring alopecia, **lichen planopilaris** is a scarring alopecia.
- Therefore, this option incorrectly groups a non-scarring and a scarring condition.
*2, 3, and 4*
- This option correctly identifies **alopecia areata** and **telogen effluvium** as non-scarring but incorrectly includes **lichen planopilaris**, which results in scarring alopecia.
- **Lichen planopilaris** has inflammatory infiltrates that lead to permanent follicular damage.
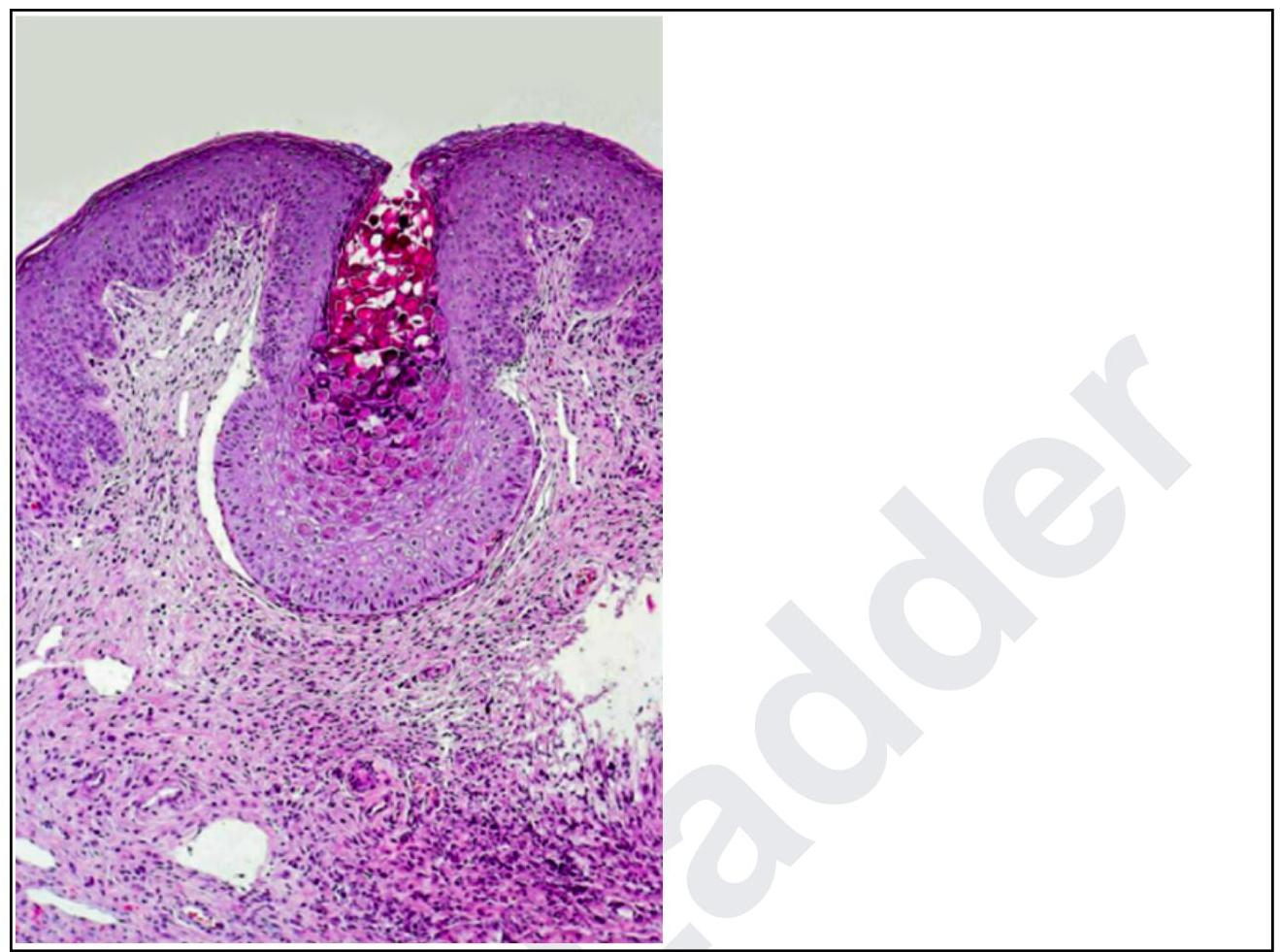
Question 5: A woman presents with lesions on the inner thighs and peri-anal region. They are nodular, 4-6 mm in size and appear pale. The histopathological image shows multiple intracytoplasmic inclusion bodies consistent with Henderson-Patterson bodies. The diagnosis is:
A. Trichodysplasia spinulosa
B. Molluscum contagiosum (Correct Answer)
C. Condyloma acuminata
D. Donovanosis
Explanation: ***Molluscum contagiosum***
- The clinical presentation of **nodular, pale lesions** in the inner thighs and peri-anal region, combined with histopathology showing **Henderson-Patterson bodies** (large eosinophilic intracytoplasmic inclusions), is pathognomonic for molluscum contagiosum.
- Henderson-Patterson bodies represent viral factories within infected keratinocytes, a key diagnostic feature of this **poxvirus** infection.
*Trichodysplasia spinulosa*
- This condition is characterized by **follicular papules** with prominent keratin spines, typically occurring on the face, and is associated with the **Trichodysplasia spinulosa-associated polyomavirus**.
- It does not present with Henderson-Patterson bodies or the typical nodular lesions seen in molluscum contagiosum.
*Condyloma acuminata*
- These are **genital warts** caused by the **human papillomavirus (HPV)**, presenting as verrucous or cauliflower-like growths.
- Histologically, they show **koilocytic atypia** (vacuolated cells with nuclear abnormalities), not Henderson-Patterson bodies.
*Donovanosis*
- Also known as **granuloma inguinale**, this is a chronic, progressive, ulcerative granulomatous disease caused by **Klebsiella granulomatis**.
- Histopathology reveals **Donovan bodies** (intracellular bacteria within macrophages), which are distinct from Henderson-Patterson bodies and the clinical presentation of nodular lesions.
Question 6: A 7-year-old child presents to the dermatology clinic with multiple small, painless, flesh-colored papules on the trunk and arms that have been present for 3 months. The lesions are 2-4 mm in diameter, dome-shaped with a smooth surface, and several have a characteristic central umbilication. The child is otherwise healthy and immunocompetent. The lesions are not pruritic and there is no associated lymphadenopathy. On closer examination, a white, cheesy material can be expressed from the central depression of some lesions.
What is the most likely diagnosis?
A. Trichodysplasia spinulosa
B. Condyloma acuminata
C. Donovanosis
D. Molluscum contagiosum (Correct Answer)
Explanation: ***Molluscum contagiosum***
- The classic presentation of **flesh-colored, dome-shaped papules** with **central umbilication** is pathognomonic for molluscum contagiosum.
- The presence of a **white, cheesy material** that can be expressed from the central depression is characteristic of the viral core.
*Trichodysplasia spinulosa*
- This condition presents with **follicular papules** and **spiny projections**, primarily on the face, and is typically seen in **immunocompromised** individuals.
- The description of **flesh-colored, dome-shaped papules** with **umbilication** does not fit the typical presentation of trichodysplasia spinulosa.
*Condyloma acuminata*
- These are **genital warts** caused by HPV, typically presenting as **verrucous** or **cauliflower-like lesions** on the anogenital region.
- The description of **small, painless, flesh-colored papules** with **central umbilication** on the trunk and arms is inconsistent with condyloma acuminata.
*Donovanosis*
- Donovanosis, or **granuloma inguinale**, is a rare bacterial infection causing **ulcerative lesions** in the genital and perianal areas.
- This diagnosis is highly unlikely given the child's age, rash location (trunk and arms), and the specific morphology of the lesions.