INI-CET 2022 — Community Medicine
12 Previous Year Questions with Answers & Explanations
Which of the following statements is true regarding the tape shown in the image?

In all the following places, hand rub can be used according to standard hand hygiene protocol, except...
As per the National Tuberculosis Elimination Program (NTEP), HIV TB prevalence of what percentage would deem a district a high priority district?
India is a country with different cultures and diverse languages. Which steps should a physician take to address the patient for better outcomes? 1. Insist on good communication 2. Insist on communication only via an interpreter 3. Treat them regardless of their cultural perceptions 4. The physician should consider the patient's religion and cultural perception Select the correct combination:
Recommended HPV vaccination schedule for 9 to 14-year-olds according to WHO SAGE guidelines is:
Which of the following is a true statement about screening tests for genetic diseases?
Which of the following is the true statement regarding measures to prevent typhoid transmission in the community?
A multivariate analysis was conducted to examine the relationship between risk of developing blindness and age. The results are shown in the table below. Which of the following is true?
Which of the following indicators can help determine whether the health system is effective at identifying leprosy cases early in the community?
Abdominal TB can occur through all of the following EXCEPT
INI-CET 2022 - Community Medicine INI-CET Practice Questions and MCQs
Question 1: Which of the following statements is true regarding the tape shown in the image?
- A. Reading of 13.5 to 14.5 cm is considered undernourished.
- B. It is called Shelter's tape.
- C. It is used to assess severe acute malnutrition. (Correct Answer)
- D. It is useful mainly for frontline field workers.
Explanation: ***It is used to assess severe acute malnutrition.*** - The tape shown is a **Mid-Upper Arm Circumference (MUAC)** tape, which is a simple and effective tool for screening children aged 6-59 months for **severe acute malnutrition (SAM)**. - The color-coded sections (red, yellow, green) on the tape directly indicate nutritional status to facilitate rapid assessment and decision-making for intervention. *Reading of 13.5 to 14.5 cm is considered undernourished.* - A MUAC reading between **11.5 cm and 12.5 cm** often indicates **moderate acute malnutrition (MAM)**, falling in the yellow zone on many MUAC tapes. - A reading of **13.5 to 14.5 cm** would typically fall in the **green zone**, indicating a **healthy nutritional status** for children aged 6-59 months, not undernourished. *It is called Shelter's tape.* - The tape shown is known as a **MUAC tape** (Mid-Upper Arm Circumference tape), not Shelter's tape. - There is no widely recognized medical assessment tool called "Shelter's tape" for nutritional assessment. *It is useful mainly for frontline field workers.* - While it is indeed a valuable tool for **frontline field workers** due to its simplicity and ease of use in community settings, it is also utilized by **healthcare professionals** in clinics and hospitals for rapid screening and assessment of malnutrition. - Its utility extends beyond just field workers, making it an essential tool in various healthcare settings, especially in low-resource environments.
Question 2: In all the following places, hand rub can be used according to standard hand hygiene protocol, except...
- A. If the hands are visibly soiled (Correct Answer)
- B. While moving from a contaminated site to a clean site during patient care
- C. During direct patient contact
- D. Before donning gloves
Explanation: ***If the hands are visibly soiled*** - **Hand rub (alcohol-based hand rub)** is ineffective at removing gross contamination and organic matter from visibly soiled hands. - In such cases, **hand washing with soap and water** is mandatory to physically remove dirt, debris, and microorganisms. *While moving from a contaminated site to a clean site during patient care* - **Hand rub** is appropriate in this scenario to prevent the transfer of microorganisms from a potentially contaminated body site or object to another, cleaner area of the patient. - This is part of the "5 Moments for Hand Hygiene" to ensure **patient safety** and prevent **cross-contamination**. *During direct patient contact* - **Hand rub** can be used before and after direct patient contact if hands are not visibly soiled, as it provides rapid and effective decontamination. - This practice is crucial for minimizing the transmission of **healthcare-associated infections**. *Before donning gloves* - **Hand rub** should be performed before donning gloves, especially when performing procedures that involve contact with mucous membranes, non-intact skin, or sterile sites. - This ensures that hands are clean underneath the gloves, providing an additional layer of **infection prevention**.
Question 3: As per the National Tuberculosis Elimination Program (NTEP), HIV TB prevalence of what percentage would deem a district a high priority district?
- A. >15 %
- B. >20 %
- C. >10 % (Correct Answer)
- D. >12 %
Explanation: ***>10%*** - As per the **National Tuberculosis Elimination Program (NTEP)** guidelines, a district is categorized as a **high-priority district** for HIV-TB co-infection if the prevalence of HIV among TB patients is **greater than 10%**. - This threshold helps in identifying regions that require enhanced focus and resources for **integrated HIV and TB care** and prevention strategies. - This is the specific cut-off defined by NTEP for prioritizing districts for targeted interventions. *>15%* - While 15% would also indicate a high prevalence, the specific threshold set by NTEP for deeming a district high priority is **>10%**, not >15%. - Districts with prevalence between 10% and 15% would already be classified as high priority at the >10% threshold. *>20%* - A prevalence of >20% would certainly indicate a severe problem, but the **NTEP's definition** for a high-priority district is specifically **>10%**. - Using a higher threshold like 20% would delay interventions in districts that already face significant challenges with HIV-TB co-infection. *>12%* - The NTEP guidelines use a specific cut-off of **>10%** for defining high-priority districts for HIV-TB co-infection. - While 12% exceeds the 10% threshold, it is not the defining threshold mentioned in the official guidelines for this classification.
Question 4: India is a country with different cultures and diverse languages. Which steps should a physician take to address the patient for better outcomes? 1. Insist on good communication 2. Insist on communication only via an interpreter 3. Treat them regardless of their cultural perceptions 4. The physician should consider the patient's religion and cultural perception Select the correct combination:
- A. 1,4 (Correct Answer)
- B. 1,2
- C. 2,3
- D. 3,4
Explanation: ***1,4*** - **Good communication** is paramount in healthcare, especially in a diverse country like India, to ensure **patient understanding**, **adherence** to treatment plans, and overall patient satisfaction. - Considering a patient's **religion and cultural perceptions** allows the physician to tailor treatment and communication in a sensitive and **respectful manner**, fostering trust and better **health outcomes**. *1,2* - While good communication (1) is vital, **insisting solely on an interpreter** (2) may not always be feasible or necessary, particularly if the physician and patient share a common language or if the patient prefers direct communication. This can also disrupt the flow of rapport building. - **Over-reliance on interpreters** can sometimes lead to misinterpretations or loss of non-verbal cues if the interpreter is not trained in medical interpretation. *2,3* - **Insisting only on an interpreter** (2) can be restrictive and may compromise direct patient-physician rapport, as discussed above. - **Treating patients regardless of their cultural perceptions** (3) is an ethnocentric approach that can lead to mistrust, non-adherence, and ultimately **poor health outcomes** as it disregards the patient's beliefs and values regarding health and illness. *3,4* - **Treating patients regardless of their cultural perceptions** (3) can result in a lack of understanding and non-adherence if the treatment conflicts with the patient's deeply held beliefs. - While considering religion and cultural perception (4) is crucial, this option includes an incorrect approach (3) that can undermine patient care.
Question 5: Recommended HPV vaccination schedule for 9 to 14-year-olds according to WHO SAGE guidelines is:
- A. 1 or 2 doses (Correct Answer)
- B. 3 doses
- C. 3 or 4 doses
- D. 4 doses
Explanation: ***1 or 2 doses*** - The **WHO Strategic Advisory Group of Experts (SAGE)** on Immunization recommends a simplified **one- or two-dose schedule** for girls and boys aged 9–14 years. - This recommendation, updated in April 2022, is based on evidence demonstrating comparable efficacy of **single-dose HPV vaccination** to multi-dose regimens in this age group, while improving accessibility and uptake. - **Key advantage**: Reduced doses improve vaccination completion rates and reduce programmatic costs without compromising protection. *3 doses* - A **three-dose schedule** (0, 1-2, 6 months) was the original recommendation but is **no longer recommended** for the 9–14 age group. - Three doses are now reserved for **immunocompromised individuals** or those starting vaccination at older ages in some guidelines. - Maintaining a three-dose schedule would increase costs and reduce completion rates unnecessarily. *3 or 4 doses* - **Four doses** have never been part of any WHO HPV vaccination recommendation. - This option represents an excessive and unsupported schedule that would create unnecessary barriers to vaccination coverage. *4 doses* - **Four doses** are not recommended by WHO SAGE for any age group or clinical scenario. - This would represent over-vaccination without evidence of additional benefit and would significantly impair program implementation.
Question 6: Which of the following is a true statement about screening tests for genetic diseases?
- A. Screening test has better accuracy than diagnostic test
- B. It is always invasive
- C. It defines risk of transmission of disease to the child (Correct Answer)
- D. Screening requires genetic mapping
Explanation: ***Correct: It defines risk of transmission of disease to the child*** - Genetic screening aims to identify individuals or couples at risk of passing on **heritable genetic conditions** to their offspring. - This information helps in **family planning** and provides prenatal diagnostic options if the risk is high. - This is the **primary purpose** of genetic screening programs. *Incorrect: Screening test has better accuracy than diagnostic test* - **Screening tests** are designed to be broad and detect potential risks, often with lower specificity and sensitivity than diagnostic tests. - **Diagnostic tests** are typically more accurate and definitive, confirming the presence or absence of a disease after a positive screening result. *Incorrect: It is always invasive* - Many genetic screening tests, such as **non-invasive prenatal screening (NIPS)** from maternal blood or carrier screening via saliva, are non-invasive or minimally invasive. - While some diagnostic tests like **amniocentesis** or **chorionic villus sampling** are invasive, screening itself is not universally so. *Incorrect: Screening requires genetic mapping* - **Genetic mapping** refers to determining the relative positions of genes on a chromosome, which is a research tool for understanding genome organization. - Genetic screening primarily involves testing for specific mutations or chromosomal abnormalities, not creating a comprehensive genetic map of an individual.
Question 7: Which of the following is the true statement regarding measures to prevent typhoid transmission in the community?
- A. Typhoid vaccine administration is the best method of preventing transmission.
- B. Person-to-person transmission is the primary mode of spread.
- C. Drug resistance in typhoid is not as big a problem as in TB.
- D. Hygiene practice and clean sanitation control are more important than the typhoid vaccine. (Correct Answer)
Explanation: ***Hygiene practice and clean sanitation control is more important than the typhoid vaccine.*** - **Improved sanitation**, safe water supplies, and adequate hygiene practices are fundamental in controlling the spread of **typhoid fever**, as the disease is primarily transmitted through the **oral-fecal route**. - While vaccines are an important tool, they offer only partial protection and must be combined with **robust public health infrastructure** and **sanitation measures** for effective prevention. *Typhoid vaccine administration is the best method of preventing transmission.* - Typhoid vaccines offer protection, but their effectiveness is not 100%, and they typically require **booster doses** - **Vaccination campaigns** are most effective when implemented alongside improvements in **water and sanitation infrastructure**, as vaccines alone cannot fully prevent transmission in areas with poor hygiene. *Person-to-person transmission is the primary mode of spread.* - While person-to-person transmission can occur, especially in settings with poor hygiene, the primary mode of spread for typhoid is through the **ingestion of food or water contaminated** with the feces of an infected person or carrier. - This emphasizes the crucial role of **water and food safety** rather than just focusing on direct person-to-person contact. *Drug resistance in typhoid is not as big a problem as in TB.* - **Antimicrobial resistance (AMR)** in typhoid fever, particularly to fluoroquinolones and extended-spectrum beta-lactamase (ESBL) producing strains, is a **significant and growing global health concern**, complicating treatment. - While TB also faces serious drug resistance issues, the escalating problem of **extensively drug-resistant (XDR)** and **multi-drug resistant (MDR)** typhoid strains makes it a substantial threat, impacting treatment options and increasing morbidity and mortality.
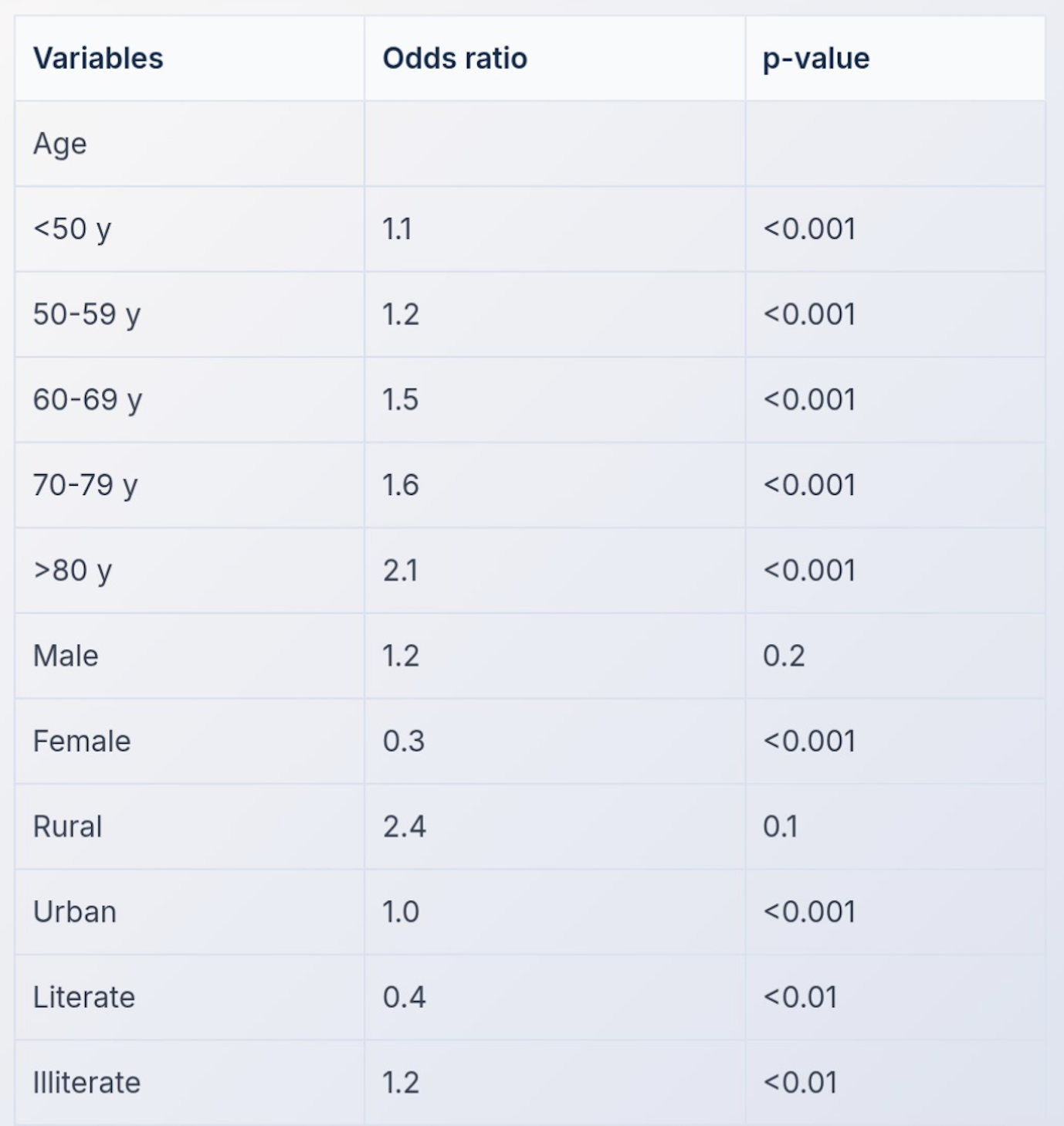
Question 8: A multivariate analysis was conducted to examine the relationship between risk of developing blindness and age. The results are shown in the table below. Which of the following is true?
- A. 60-69 y age group shows statistically significant association with blindness
- B. <50 y age group serves as the reference category
- C. >80 y age group has the strongest association with blindness risk (Correct Answer)
- D. 50-59 y age group has the highest odds ratio for blindness risk
Explanation: ***>80 y age group has the strongest association with blindness risk*** - The odds ratio for the **>80 years** age group is **2.1**, which is the highest among all age groups listed in the table, indicating the strongest association with blindness risk. - A higher odds ratio means a greater likelihood of the outcome (blindness) compared to the reference category. - All age groups shown have **p-values <0.001**, confirming statistical significance. *60-69 y age group shows statistically significant association with blindness* - While the 60-69 y age group has an odds ratio of **1.5** with **p<0.001**, indicating statistical significance, it does not have the strongest association compared to the **>80 y** age group (OR 2.1). - Statistical significance confirms the association is real, but effect size (OR) determines strength of association. *<50 y age group serves as the reference category* - The table shows an **Odds Ratio (OR) of 1.1** for the **<50 y** age group, indicating it is also being compared to a reference (which would have OR = 1.0). - The reference category is not explicitly shown in the table but would typically be an even younger age group or overall population baseline. *50-59 y age group has the highest odds ratio for blindness risk* - The odds ratio for the **50-59 y** age group is **1.2**, which is lower than the **>80 y** age group (OR 2.1), the **70-79 y** age group (OR 1.6), and the **60-69 y** age group (OR 1.5). - This statement is incorrect as the **>80 y** age group clearly has the highest odds ratio for blindness risk.
Question 9: Which of the following indicators can help determine whether the health system is effective at identifying leprosy cases early in the community?
- A. Proportion of newly diagnosed patients with grade 2 disability (Correct Answer)
- B. Annual new case detection rate per lac
- C. Treatment initiation rate
- D. Treatment completion rate
Explanation: ***Proportion of newly diagnosed patients with grade 2 disability*** - A **high proportion of newly diagnosed patients with grade 2 disability** indicates late detection of leprosy, suggesting shortcomings in the health system's ability to identify cases early. - Grade 2 disability in leprosy signifies **visible and irreversible damage** to eyes, hands, or feet, which would likely have been prevented with earlier diagnosis and treatment. *Annual new case detection rate per lac* - The **annual new case detection rate** reflects the number of new cases identified but does not directly indicate the timeliness of detection or the effectiveness of early case-finding efforts. - A high new case detection rate could be due to intensive active case-finding campaigns, but without knowing the disability status at diagnosis, it doesn't confirm early detection by the routine health system. *Treatment initiation rate* - The **treatment initiation rate** measures the percentage of diagnosed patients who start treatment, which is crucial for disease control but does not reflect how early cases are identified. - A high initiation rate indicates good patient adherence to treatment protocols after diagnosis, but not the efficiency of the health system in finding cases before they develop advanced disability. *Treatment completion rate* - The **treatment completion rate** indicates the effectiveness of the treatment program and patient adherence, which is vital for preventing drug resistance and relapse. - This metric does not provide information about when the diagnosis was made in the disease progression or the health system's ability to identify cases early.
Question 10: Abdominal TB can occur through all of the following EXCEPT
- A. Direct spread from mesenteric lymph nodes
- B. Feco - oral route
- C. Direct contact with infected animal (Correct Answer)
- D. Hematogenous spread
Explanation: ***Direct contact with infected animal*** - While animal products like **unpasteurized milk** can transmit *Mycobacterium bovis* to humans, direct contact with an infected animal is not a primary mode of transmission for **abdominal TB**. - **Abdominal TB** is usually caused by *Mycobacterium tuberculosis* which is primarily a human pathogen, not typically transmitted through direct contact with animals. *Direct spread from mesenteric lymph nodes* - **Mesenteric lymph nodes** are often involved in abdominal TB, and the infection can directly spread from these nodes to adjacent abdominal organs. - This is a common mechanism for localized propagation within the abdominal cavity. *Feco - oral route* - The **ingestion of contaminated food or milk** (from infected cattle) containing *Mycobacterium bovis* or swallowing of **infected sputum** (from pulmonary TB) containing *Mycobacterium tuberculosis* are common ways the bacteria can reach the gastrointestinal tract. - This leads to primary intestinal infection or reactivation of previously ingested bacteria. *Hematogenous spread* - **Hematogenous dissemination** from a primary pulmonary or other mycobacterial focus is a significant mode of transmission for abdominal TB. - Bacteria can travel through the bloodstream and seed distant abdominal organs, including the **peritoneum**, **intestines**, or **mesenteric lymph nodes**.