INI-CET 2022 — Anatomy
15 Previous Year Questions with Answers & Explanations
What is the volume of the prostate in normal adult males?
Which ligament connects medial cuneiform to the base of the 2nd metatarsal?
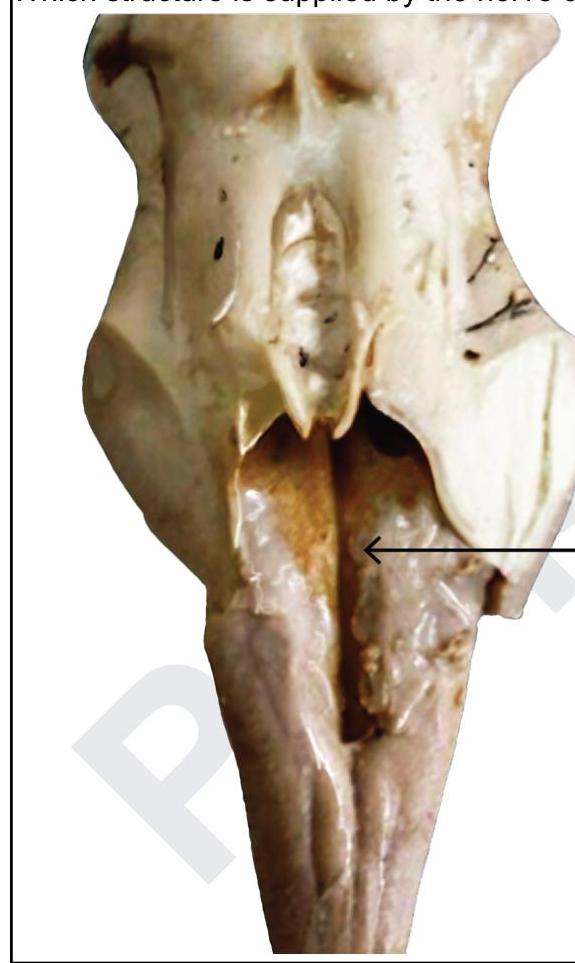
Which structure is supplied by the nerve causing this elevation?
Arrange lung hilar structure from anterior to posterior:- 1. Primary bronchus 2. Bronchial artery 3. Pulmonary vein 4. Pulmonary artery
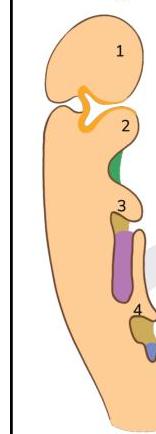
A child lacks thymus and inferior parathyroid glands. Defective development of which of the following structures is likely to be the cause?
Arrange the cells according to their positions from the basal layer towards the lumen in the seminiferous tubules:- 1. Spermatogonia 2. Primary spermatocyte 3. Spermatid 4. Spermatozoa
Identify the incorrect statement regarding the marked structure.
Arrange the following in the sequence of auditory pathway: 1. Cochlear nucleus 2. Spiral ganglion 3. Superior olivary nucleus 4. Inferior colliculus 5. Medial geniculate body
What is the action of the superior oblique muscle?
A pregnant woman presents with fever, retroorbital pain, headache, pulsatile proptosis of the right eye, and tinnitus. BP and fundus were normal. Which of the following structures are involved?
INI-CET 2022 - Anatomy INI-CET Practice Questions and MCQs
Question 1: What is the volume of the prostate in normal adult males?
- A. 50cc
- B. 75cc
- C. 100cc
- D. 20cc (Correct Answer)
Explanation: ***20cc*** - The normal prostate volume in adult males is typically **20 cubic centimeters (cc)** or grams, which is approximately the size of a walnut. - This volume is generally used as a baseline when assessing for conditions like **benign prostatic hyperplasia (BPH)** or prostate cancer, where an enlarged prostate is a key indicator [1]. *50cc* - A prostate volume of 50cc is considered **enlarged** and is often indicative of **benign prostatic hyperplasia (BPH)**, especially in older men [1]. - This volume would lead to symptoms of **lower urinary tract symptoms (LUTS)**, such as frequent urination or difficulty voiding, which are not characteristic of a normal prostate [1]. *75cc* - A prostate volume of 75cc represents a **significantly enlarged prostate**, well beyond the normal range. - Such a size would almost certainly be associated with **moderate to severe LUTS** and likely require medical intervention for BPH. *100cc* - A 100cc prostate is considered a **markedly enlarged prostate**, typically resulting in severe **urinary obstruction** and significant impact on quality of life. - This volume is far from normal and would usually necessitate treatment for **benign prostatic hyperplasia (BPH)**.
Question 2: Which ligament connects medial cuneiform to the base of the 2nd metatarsal?
- A. Chopart
- B. Deltoid
- C. Lisfranc (Correct Answer)
- D. Spring
Explanation: ***Lisfranc*** - The **Lisfranc ligament** specifically connects the medial cuneiform to the base of the second metatarsal, forming a crucial part of the **tarsometatarsal joint complex**. - Its strength and integrity are vital for **midfoot stability**, and injury to this ligament can lead to significant functional impairment. *Chopart* - The **Chopart joint** (transverse tarsal joint) involves the talonavicular and calcaneocuboid articulations. - While it is a significant midfoot joint, it does not directly connect the medial cuneiform to the second metatarsal. *Deltoid* - The **deltoid ligament** is located on the medial side of the ankle, connecting the tibia to the talus, calcaneus, and navicular bones. - It primarily provides stability to the **ankle joint** and is not involved in hindfoot-to-midfoot connections. *Spring* - The **spring ligament** (plantar calcaneonavicular ligament) connects the calcaneus to the navicular bone. - It plays a crucial role in supporting the **medial longitudinal arch** of the foot, but does not connect the cuneiform to the metatarsals.
Question 3: Which structure is supplied by the nerve causing this elevation?
- A. Risorius
- B. Masseter
- C. Lateral rectus
- D. Superior oblique (Correct Answer)
Explanation: ***Superior oblique*** - The **trochlear nerve (CN IV)** causes the elevation visible in the image at the **dorsal midbrain** level, supplying the **superior oblique muscle**. - This nerve is unique as it **decussates completely** and has the longest intracranial course, making it prone to injury. *Risorius* - The **risorius muscle** is innervated by the **facial nerve (CN VII)**, which exits at the **pontomedullary junction**. - This nerve does not cause elevations at the **dorsal midbrain** level where the arrow is pointing. *Masseter* - The **masseter muscle** is one of the muscles of mastication innervated by the **mandibular division of the trigeminal nerve (CN V)**. - The trigeminal nerve has its motor nucleus in the **pons**, not at the dorsal midbrain level where the elevation is visible in the image. *Lateral rectus* - The **lateral rectus muscle** is supplied by the **abducens nerve (CN VI)**, which exits at the **pontomedullary sulcus**. - The abducens nerve pathway does not create the elevation seen at the **dorsal midbrain** in this image.
Question 4: Arrange lung hilar structure from anterior to posterior:- 1. Primary bronchus 2. Bronchial artery 3. Pulmonary vein 4. Pulmonary artery
- A. 4,3,2,1
- B. 3,4,1,2 (Correct Answer)
- C. 1,2,3,4
- D. 2,3,4,1
Explanation: ***3,4,1,2*** - This order represents the typical arrangement of major structures in the **lung hilum** from anterior to posterior: **pulmonary vein (most anterior)**, **pulmonary artery**, **primary bronchus**, and finally the **bronchial artery (most posterior)**. - The **pulmonary vein** is usually the most anterior structure, while the **bronchial artery** often runs along the posterior aspect of the bronchus [1]. *4,3,2,1* - This order incorrectly places the **pulmonary artery** as the most anterior structure, which is generally not the case in the hilum. - The **primary bronchus** is usually more posterior than the main pulmonary artery. *1,2,3,4* - This order is incorrect as it places the **primary bronchus** as the most anterior structure, which is anatomically inaccurate for the lung hilum. - The **pulmonary veins** are typically the most anterior hilar structures. *2,3,4,1* - This order incorrectly positions the **bronchial artery** as the most anterior component, while it is usually the most posterior or associated closely with the posterior aspect of the bronchus. - The **pulmonary vein** should be anterior to the pulmonary artery and bronchus.
Question 5: A child lacks thymus and inferior parathyroid glands. Defective development of which of the following structures is likely to be the cause?
- A. 2
- B. 4
- C. 1
- D. 3 (Correct Answer)
Explanation: ***Option 3 (Structure 3 - Third pharyngeal pouch)*** - Structure **3** represents the **third pharyngeal pouch**, which is the embryological origin of both the **thymus** and **inferior parathyroid glands**. - Defective development of the third pharyngeal pouch leads to **DiGeorge syndrome** (22q11.2 deletion syndrome), characterized by thymic hypoplasia/aplasia and hypoparathyroidism. - This explains the clinical presentation of absent thymus and inferior parathyroid glands. *Option 2 (Structure 2 - Second pharyngeal pouch)* - Structure **2** represents the **second pharyngeal pouch**. - This gives rise to the **palatine tonsils** and the **tonsillar fossa**. - Not related to thymus or parathyroid gland development. *Option 1 (Structure 1 - First pharyngeal pouch)* - Structure **1** represents the **first pharyngeal pouch**. - This develops into the **eustachian tube** (auditory tube) and **middle ear cavity** (tympanic cavity). - Not related to thymus or inferior parathyroid gland development. *Option 4 (Structure 4 - Fourth pharyngeal pouch)* - Structure **4** represents the **fourth pharyngeal pouch**. - This gives rise to the **superior parathyroid glands** (dorsal wing) and **ultimobranchial body** (ventral wing), which contributes parafollicular C cells to the thyroid gland. - Note: The inferior parathyroids (from 3rd pouch) migrate further caudally than superior parathyroids (from 4th pouch).
Question 6: Arrange the cells according to their positions from the basal layer towards the lumen in the seminiferous tubules:- 1. Spermatogonia 2. Primary spermatocyte 3. Spermatid 4. Spermatozoa
- A. 2,1,3,4
- B. 1,2,3,4 (Correct Answer)
- C. 1,3,2,4
- D. 4,3,2,1
Explanation: ***1,2,3,4*** - This sequence accurately represents the **developmental progression of male germ cells** from the basal lamina towards the lumen of the seminiferous tubule [1], [2]. - **Spermatogonia** are stem cells located near the basal lamina [1], which then differentiate into **primary spermatocytes**, followed by **spermatids**, and finally maturing into **spermatozoa** that are released into the lumen [2]. *2,1,3,4* - This order is incorrect because **primary spermatocytes** develop from spermatogonia [2], meaning spermatogonia should precede primary spermatocytes in the sequence. - The initial cell in the spermatogenic lineage is the **spermatogonium**, found at the base of the tubule [1]. *1,3,2,4* - This sequence is incorrect as **primary spermatocytes** undergo meiosis to form secondary spermatocytes, which then become spermatids [2]. - Therefore, **spermatids** develop *after* primary spermatocytes, not before them. *4,3,2,1* - This order is a reversal of the actual developmental process and spatial arrangement within the seminiferous tubule. - **Spermatozoa** are the most mature cells and are found closest to the lumen [1], while **spermatogonia** are located at the basal layer [1].
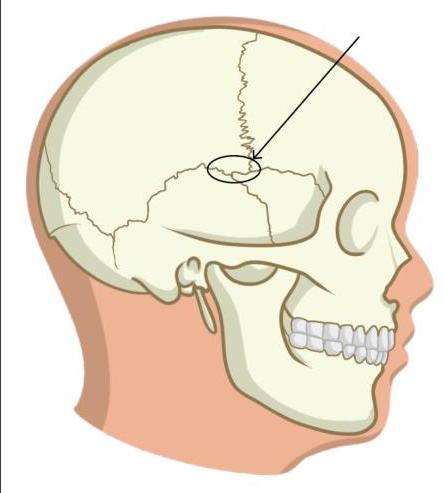
Question 7: Identify the incorrect statement regarding the marked structure.
- A. It is the meeting point of frontal, parietal, temporal and sphenoid bones.
- B. Accessory middle meningeal artery lies under this structure (Correct Answer)
- C. Blow to the lateral side of the skull injures the marked structure
- D. It corresponds to site of anterolateral fontanelle of fetal skull
Explanation: *It is the meeting point of frontal, parietal, temporal and sphenoid bones.* - The marked structure is the **pterion**, which is indeed the junction of the **frontal, parietal, temporal, and sphenoid bones**. - This statement is **correct**, as it accurately describes the anatomical composition of the pterion. ***Accessory middle meningeal artery lies under this structure*** - This is the **INCORRECT statement** and hence the correct answer. - The **middle meningeal artery** (not the accessory middle meningeal artery) runs in a groove deep to the pterion. - A fracture at the pterion can lacerate the **middle meningeal artery**, leading to an **epidural hematoma**. - The accessory middle meningeal artery is a separate vessel that does not typically lie under the pterion. *Blow to the lateral side of the skull injures the marked structure* - The pterion is the **thinnest part of the lateral wall of the skull**, making it vulnerable to fracture from a lateral blow. - Due to its thinness and underlying structures, trauma to this area is clinically significant. - This statement is **correct**. *It corresponds to site of anterolateral fontanelle of fetal skull* - The pterion in the adult skull corresponds to the former site of the **anterolateral (sphenoidal) fontanelle** in the fetal skull. - This fontanelle allows for skull molding during birth and brain growth postnatally. - This statement is **correct**.
Question 8: Arrange the following in the sequence of auditory pathway: 1. Cochlear nucleus 2. Spiral ganglion 3. Superior olivary nucleus 4. Inferior colliculus 5. Medial geniculate body
- A. 5-4-3-2-1
- B. 3-4-5-1-2
- C. 2-1-3-4-5 (Correct Answer)
- D. 1-2-3-4-5
Explanation: ***2-1-3-4-5*** - The auditory pathway begins with the **spiral ganglion**, which contains the cell bodies of the first-order neurons that innervate the hair cells of the cochlea. - Signals then proceed to the **cochlear nucleus** in the brainstem, followed by the **superior olivary nucleus**, the **inferior colliculus**, and finally the **medial geniculate body** in the thalamus before reaching the auditory cortex [1]. *5-4-3-2-1* - This sequence represents a nearly reverse order of the ascending auditory pathway, starting from a higher processing center (medial geniculate body) and moving backward, which is incorrect for sensory input. - The **medial geniculate body** is the thalamic relay for auditory information, receiving input from lower centers and projecting to the auditory cortex [1]. *3-4-5-1-2* - This sequence incorrectly places the **superior olivary nucleus** as the initial processing stage, preceding the lower-level **spiral ganglion** and **cochlear nucleus**. - Auditory information must first be transduced by hair cells and then relayed by the spiral ganglion neurons to the cochlear nucleus before further processing in the olivary complex. *1-2-3-4-5* - This sequence incorrectly places the **cochlear nucleus** before the **spiral ganglion**. - The **spiral ganglion** contains the primary afferent neurons that receive input from the hair cells and project their axons to the cochlear nucleus.
Question 9: What is the action of the superior oblique muscle?
- A. Intorsion, adduction, elevation
- B. Extorsion, adduction, elevation
- C. Extorsion, abduction, depression
- D. Intorsion, abduction, depression (Correct Answer)
Explanation: ***Intorsion, abduction, depression*** - The **superior oblique muscle** has three actions: **depression** (downward movement - primary action), **abduction** (movement away from the midline), and **intorsion** (medial/internal rotation of the globe) [1]. - The depressor action is most effective when the eye is **adducted** (turned inward), as the muscle's line of pull is then optimally aligned with the vertical axis. - Mnemonic: **SO-DAI** (Superior Oblique: Depression, Abduction, Intorsion) *Intorsion, adduction, elevation* - While **intorsion** is correct, this option incorrectly includes **adduction** and **elevation**. - The superior oblique causes **abduction** (not adduction) and **depression** (not elevation) [1]. - **Elevation** is performed by the superior rectus and inferior oblique muscles [1]. *Extorsion, adduction, elevation* - All three actions are incorrect for the superior oblique muscle. - The correct actions are **intorsion**, **abduction**, and **depression**. - **Extorsion** is performed by the inferior oblique and inferior rectus muscles [1]. *Extorsion, abduction, depression* - While **abduction** and **depression** are correct, **extorsion** is wrong. - The superior oblique causes **intorsion** (internal rotation), not extorsion (external rotation). - This is a common point of confusion - remember the superior oblique **intorts**, while the inferior oblique **extorts**.
Question 10: A pregnant woman presents with fever, retroorbital pain, headache, pulsatile proptosis of the right eye, and tinnitus. BP and fundus were normal. Which of the following structures are involved?
- A. Oculomotor nerve, Internal carotid artery, Cavernous sinus
- B. Abducens nerve, Internal carotid artery, Cavernous sinus
- C. Abducens nerve, Oculomotor nerve, Internal carotid artery
- D. Abducens nerve, Oculomotor nerve, Internal carotid artery, Cavernous sinus (Correct Answer)
Explanation: Abducens nerve, Oculomotor nerve, Internal carotid artery, Cavernous sinus - The combination of retroorbital pain, pulsatile proptosis, and tinnitus in a pregnant woman (indicating a potential hypercoagulable state) strongly suggests a carotid-cavernous fistula. - A carotid-cavernous fistula directly connects the high-pressure internal carotid artery to the low-pressure cavernous sinus, causing engorgement of the sinus and venous backflow. This can directly impact structures passing through or adjacent to the cavernous sinus, explaining the range of symptoms. - The oculomotor nerve (CN III) and abducens nerve (CN VI) both traverse the cavernous sinus and are commonly affected, leading to ophthalmoplegia and cranial nerve palsies. Abducens nerve, Oculomotor nerve, Internal carotid artery - This option incorrectly omits the cavernous sinus, which is central to the pathophysiology of the symptoms presented. - The cavernous sinus is the anatomical location where the internal carotid artery and multiple cranial nerves (including abducens and oculomotor) are in close proximity, making its involvement crucial for the observed signs. Oculomotor nerve, Internal carotid artery, Cavernous sinus - This option incorrectly omits the abducens nerve. While not explicitly stated as palsy, this nerve is often affected alongside the oculomotor nerve due to its passage through the cavernous sinus. - Involvement of the cavernous sinus often leads to dysfunction of cranial nerves III, IV, V1, V2, and VI, making abducens nerve involvement highly probable in such cases. Abducens nerve, Internal carotid artery, Cavernous sinus - This option incorrectly omits the oculomotor nerve. Pulsatile proptosis and retroorbital pain are strong indicators of cavernous sinus pathology, which frequently involves the oculomotor nerve (CN III), leading to ophthalmoplegia or partial palsies. - The oculomotor nerve is particularly vulnerable due to its course within the lateral wall of the cavernous sinus, making its involvement a common finding in cavernous sinus disorders.