INI-CET 2022
157 Previous Year Questions with Answers & Explanations
Biochemistry
1 questionsMatch the following molecules with their carriers in plasma: MOLECULES: 1. Thyroxine 2. Fatty acid 3. Hemoglobin 4. Heme CARRIERS: A. Hemopexin B. Prealbumin C. Albumin D. Haptoglobin
INI-CET 2022 - Biochemistry INI-CET Practice Questions and MCQs
Question 1: Match the following molecules with their carriers in plasma: MOLECULES: 1. Thyroxine 2. Fatty acid 3. Hemoglobin 4. Heme CARRIERS: A. Hemopexin B. Prealbumin C. Albumin D. Haptoglobin
- A. 1-B, 2-C, 3-A, 4-D
- B. 1-A, 2-B, 3-C, 4-D
- C. 1-B, 2-C, 3-D, 4-A (Correct Answer)
- D. 1-A, 2-D, 3-B, 4-C
Explanation: ***1-B, 2-C, 3-D, 4-A*** - **Thyroxine** is primarily transported by **prealbumin (transthyretin)**, which has high affinity for thyroid hormones and prevents their rapid clearance. - **Fatty acids** bind to **albumin** at multiple binding sites, allowing efficient transport of these hydrophobic molecules in plasma. - **Hemoglobin** released from lysed red blood cells is bound by **haptoglobin** to prevent renal loss and iron wastage. - **Heme** groups are specifically transported by **hemopexin**, which has the highest binding affinity for heme among plasma proteins. *1-B, 2-C, 3-A, 4-D* - Incorrectly pairs **hemoglobin** with hemopexin; hemoglobin binds to **haptoglobin** to form stable complexes. - Incorrectly pairs **heme** with haptoglobin; free heme has highest affinity for **hemopexin**, not haptoglobin. *1-A, 2-B, 3-C, 4-D* - Incorrectly pairs **thyroxine** with hemopexin; thyroxine is primarily carried by **prealbumin** and thyroxine-binding globulin. - Incorrectly pairs **fatty acids** with prealbumin; fatty acids bind predominantly to **albumin** due to its multiple hydrophobic binding sites. *1-A, 2-D, 3-B, 4-C* - Incorrectly pairs **heme** with albumin; while albumin can bind heme weakly, **hemopexin** is the specific high-affinity carrier. - Incorrectly pairs **hemoglobin** with prealbumin; free hemoglobin forms specific complexes with **haptoglobin** for recycling.
Internal Medicine
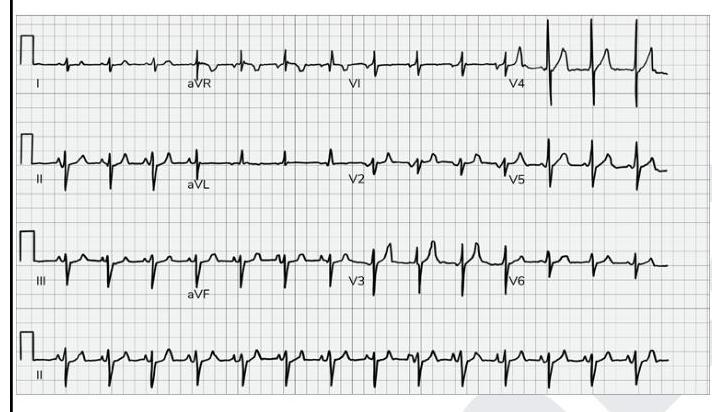
2 questionsWhat does the given ECG show?
Which of the following statements are true about familial adenomatous polyposis? 1. It is autosomal recessive 2. If not treated, 100% of the cases progress to adenocarcinoma colon. 3. It is associated with a gene mutation in KRAS 4. It is associated with congenital hypertrophy of the retinal pigment epithelium.
INI-CET 2022 - Internal Medicine INI-CET Practice Questions and MCQs
Question 1: What does the given ECG show?
- A. P-pulmonale (Correct Answer)
- B. Improper calibration
- C. Electrical alternans
- D. Ventricular bigeminy
Explanation: ***P-pulmonale*** - The ECG shows tall, peaked **P waves** with an amplitude of more than **2.5 mm in lead II**, which is characteristic of P-pulmonale. - P-pulmonale indicates **right atrial enlargement or hypertrophy**, often due to conditions like severe lung disease (e.g., COPD) or pulmonary hypertension. *Improper calibration* - Improper calibration would typically affect the amplitude of all ECG complexes globally or specific leads consistently, which is not the primary finding here. - The calibration mark (first beat in lead I) appears normal, indicating standard calibration (10mm/mV). *Electrical alternans* - **Electrical alternans** is characterized by beat-to-beat variation in the QRS complex amplitude, which is not visible in this ECG. - It is commonly associated with **pericardial effusion with cardiac tamponade**. *Ventricular bigeminy* - **Ventricular bigeminy** is a pattern where every normal sinus beat is followed by a premature ventricular contraction (PVC). - This ECG shows a regular rhythm with consistent P-QRS-T morphology, without alternating normal and PVC beats.
Question 2: Which of the following statements are true about familial adenomatous polyposis? 1. It is autosomal recessive 2. If not treated, 100% of the cases progress to adenocarcinoma colon. 3. It is associated with a gene mutation in KRAS 4. It is associated with congenital hypertrophy of the retinal pigment epithelium.
- A. 2 and 4 (Correct Answer)
- B. None of the options
- C. 1 and 4
- D. 2 and 3
Explanation: ***2 and 4*** - Without treatment, **familial adenomatous polyposis (FAP)** leads to colorectal **adenocarcinoma** in 100% of cases, due to the accumulation of numerous adenomatous polyps throughout the colon. - FAP is strongly associated with **congenital hypertrophy of the retinal pigment epithelium (CHRPE)**, which can be an early diagnostic marker [1]. *None of the options* - This statement is incorrect because FAP does indeed involve the progression to adenocarcinoma and is associated with CHRPE. - The combination of these two true statements makes this option invalid. *1 and 4* - FAP is inherited in an **autosomal dominant** manner, not autosomal recessive [1]. - While statement 4 (association with CHRPE) is true, statement 1 being false makes this option incorrect. *2 and 3* - Although statement 2 (100% progression to adenocarcinoma) is true, statement 3 is incorrect. - FAP is primarily caused by mutations in the **APC gene**, not the KRAS gene [1]. KRAS is more commonly associated with sporadic colorectal cancer progression rather than FAP.
Pathology
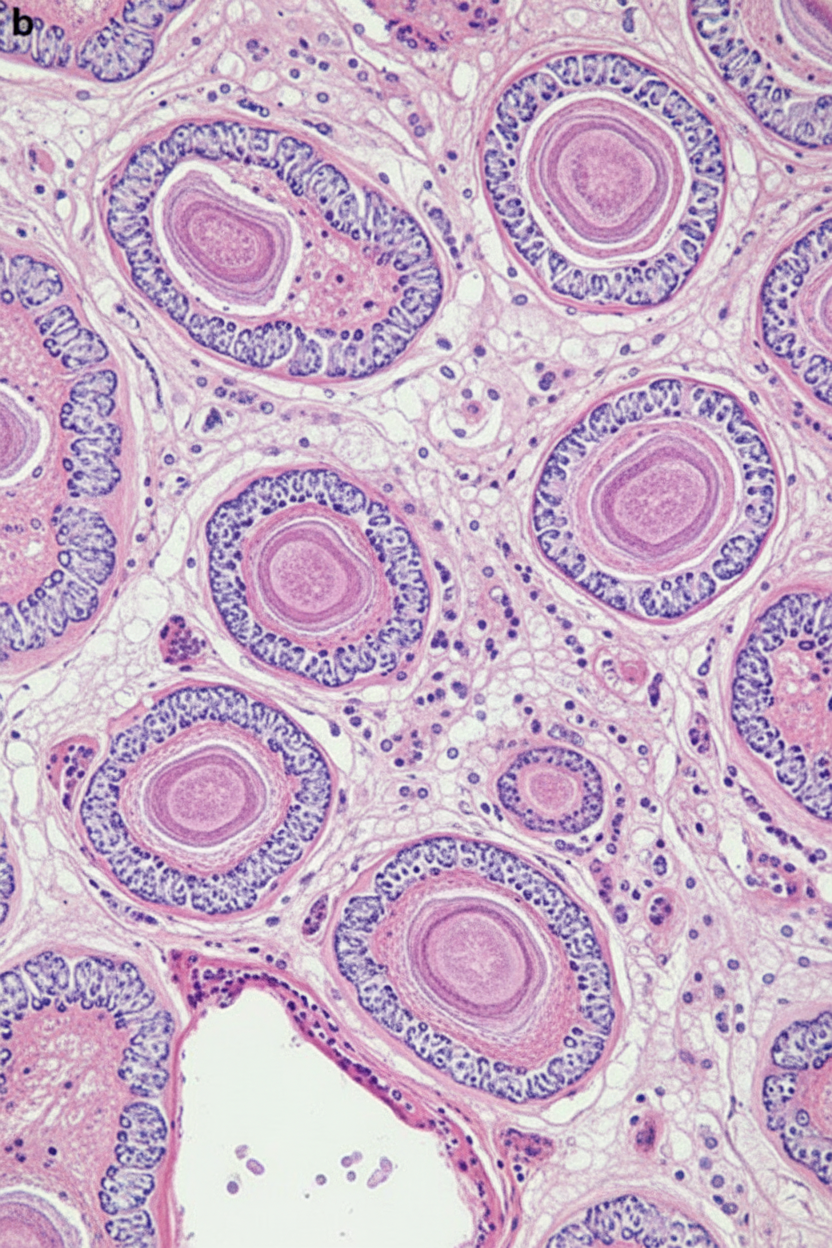
1 questionsA male patient with hemoptysis. On examination, hilar mass was present. The histopathological image is shown below. Immunohistochemistry revealed that the cells were positive for p40. What is the diagnosis?
INI-CET 2022 - Pathology INI-CET Practice Questions and MCQs
Question 1: A male patient with hemoptysis. On examination, hilar mass was present. The histopathological image is shown below. Immunohistochemistry revealed that the cells were positive for p40. What is the diagnosis?
- A. Squamous cell carcinoma (Correct Answer)
- B. Adenocarcinoma lung
- C. Small cell carcinoma
- D. Large cell carcinoma
Explanation: ***Squamous cell carcinoma*** - The image displays features characteristic of **squamous cell carcinoma**, including nests of polygonal cells, prominent nucleoli, and areas of **keratinization** (forming keratin pearls) which are indicative of squamous differentiation [1]. - The positive immunohistochemistry staining for **p40** is a highly specific marker for squamous cell differentiation, further confirming the diagnosis in the context of a hilar mass and hemoptysis, which are common presentations for this type of lung cancer [2]. *Adenocarcinoma lung* - **Adenocarcinoma lung** typically presents with glandular differentiation, featuring structures like acini, tubules, or papillae, and often produces mucin, none of which are evident in the provided image [1]. - Immunohistochemically, adenocarcinoma would typically stain positive for **TTF-1** or **Napsin A**, and would be negative for p40. *Small cell carcinoma* - **Small cell carcinoma** shows small, round to oval cells with scant cytoplasm, finely granular chromatin (salt and pepper pattern), and frequent mitoses with extensive necrosis [3]. - These cells are much smaller than squamous cells and lack keratinization. IHC would show positivity for **synaptophysin, chromogranin, and CD56** (neuroendocrine markers), not p40 [3]. *Large cell carcinoma* - **Large cell carcinoma** is a diagnosis of exclusion showing undifferentiated large cells without glandular or squamous differentiation features. - It lacks the keratinization and intercellular bridges seen here, and would be **p40 negative** as it shows no squamous differentiation. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 723-724. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 336-337. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 337-338.
Pharmacology
3 questionsMatch the following drugs in Column A with their contraindications in Column B. | Column A | Column B | | :-- | :-- | | 1. Morphine | 1. QT prolongation | | 2. Amiodarone | 2. Thromboembolism | | 3. Vigabatrin | 3. Pregnancy | | 4. Estrogen preparations | 4. Head injury |
Which among the following is the false statement regarding statins?
Choose the correctly matched pairs regarding the drugs used in schizophrenia: 1. D2 antagonism: Reduces positive symptoms 2. 5HT2A antagonism: Reduces negative symptoms 3. 5HT1A agonism: Weight loss 4. Muscarinic antagonism: Reduces extrapyramidal symptoms
INI-CET 2022 - Pharmacology INI-CET Practice Questions and MCQs
Question 1: Match the following drugs in Column A with their contraindications in Column B. | Column A | Column B | | :-- | :-- | | 1. Morphine | 1. QT prolongation | | 2. Amiodarone | 2. Thromboembolism | | 3. Vigabatrin | 3. Pregnancy | | 4. Estrogen preparations | 4. Head injury |
- A. A-1, B-3, C-2, D-4
- B. A-4, B-1, C-3, D-2 (Correct Answer)
- C. A-3, B-2, C-4, D-1
- D. A-2, B-4, C-1, D-3
Explanation: ***A-4, B-1, C-3, D-2*** - **Morphine** is contraindicated in **head injury** as it can increase intracranial pressure and mask neurological symptoms. - **Amiodarone** is contraindicated in patients with **QT prolongation** due to its risk of inducing more severe arrhythmias like Torsades de Pointes. - **Vigabatrin** is contraindicated during **pregnancy** due to its potential for teratogenicity and adverse effects on fetal development. - **Estrogen preparations** are contraindicated in patients with a history of **thromboembolism** due to their increased risk of blood clot formation. *A-1, B-3, C-2, D-4* - This option incorrectly matches **Morphine** with QT prolongation and **Estrogen preparations** with head injury, which are not their primary contraindications. - It also incorrectly links **Vigabatrin** with thromboembolism and **Amiodarone** with pregnancy. *A-3, B-2, C-4, D-1* - This choice incorrectly associates **Morphine** with pregnancy and **Vigabatrin** with head injury, which are not the most critical or direct contraindications. - It also misaligns **Amiodarone** with thromboembolism and **Estrogen preparations** with QT prolongation. *A-2, B-4, C-1, D-3* - This option incorrectly matches **Morphine** with thromboembolism and **Amiodarone** with head injury, which are not their most significant contraindications. - It also incorrectly links **Vigabatrin** with QT prolongation and **Estrogen preparations** with pregnancy.
Question 2: Which among the following is the false statement regarding statins?
- A. These drugs should not be stopped even in severe conditions like injury, surgery etc.
- B. Although HMG-CoA reductase inhibitors substantially reduce the risk of cardiovascular events, there is mild increase in lipoprotein a (Lpa) levels.
- C. With the long term use, there is slight increase in the incidence of type 2 diabetes mellitus.
- D. They can be given with verapamil and other enzyme inhibitors (Correct Answer)
Explanation: ***They can be given with verapamil and other enzyme inhibitors*** - This statement is **FALSE** and is the correct answer because **verapamil** (a moderate CYP3A4 inhibitor) and other potent CYP3A4 inhibitors like **clarithromycin** or **azole antifungals** can significantly increase statin concentrations, raising the risk of adverse effects like **myopathy** and **rhabdomyolysis**. - **Co-administration** of statins with these inhibitors generally requires careful dose adjustments or avoidance, as they increase the systemic exposure to most statins (especially **simvastatin**, **atorvastatin**, and **lovastatin**). *These drugs should not be stopped even in severe conditions like injury, surgery etc.* - This statement could be considered false in certain contexts, as statins **can be temporarily held** in acute, severe conditions like sepsis, major trauma, or complex surgery, especially if there's a concern for **acute kidney injury** or **rhabdomyolysis** [1]. - However, in most routine surgical situations, statins are typically continued due to their cardiovascular protective effects. *Although HMG-CoA reductase inhibitors substantially reduce the risk of cardiovascular events, there is mild increase in lipoprotein a (Lpa) levels.* - This statement is **TRUE**. Statins are associated with a **modest increase in Lp(a) levels** (approximately 10-20%), which has been consistently demonstrated in clinical studies [2]. - While statins effectively lower **LDL cholesterol**, Lp(a) levels are largely **genetically determined** and may paradoxically increase with statin therapy, though this effect is generally considered clinically insignificant compared to the overall cardiovascular benefits [2]. *With the long term use, there is slight increase in the incidence of type 2 diabetes mellitus.* - This statement is **TRUE**. Long-term statin use is associated with a **small but statistically significant increase** in the risk of developing **type 2 diabetes mellitus** (approximately 9-12% increased risk), particularly in individuals with pre-existing risk factors like **metabolic syndrome**. - This risk, however, is generally **outweighed by the cardiovascular benefits** of statin therapy in at-risk patients, making it an acceptable trade-off.
Question 3: Choose the correctly matched pairs regarding the drugs used in schizophrenia: 1. D2 antagonism: Reduces positive symptoms 2. 5HT2A antagonism: Reduces negative symptoms 3. 5HT1A agonism: Weight loss 4. Muscarinic antagonism: Reduces extrapyramidal symptoms
- A. 1,4
- B. 1,2,4
- C. 1,2,3,4
- D. 1,2 (Correct Answer)
Explanation: ***1,2*** - **D2 antagonism** is the primary mechanism by which antipsychotics reduce **positive symptoms** of schizophrenia, such as hallucinations and delusions. - **5HT2A antagonism** is a key mechanism of atypical antipsychotics contributing to the reduction of **negative symptoms** (e.g., apathy, anhedonia, flat affect) and cognitive deficits, while also reducing the risk of extrapyramidal symptoms. *1,2,3,4* - This option is incorrect because **5HT1A agonism** is not associated with **weight loss**. While 5HT1A partial agonism (as seen with aripiprazole and brexpiprazole) may improve negative symptoms, anxiety, and cognitive function, it does not directly cause weight loss. - Additionally, **muscarinic antagonism** does not reduce extrapyramidal symptoms as a primary mechanism. Rather, anticholinergic (muscarinic antagonist) drugs like benztropine are used to **treat** EPS after it occurs. The reduction of EPS in atypical antipsychotics primarily comes from 5HT2A antagonism and lower D2 binding affinity. *1,2,4* - This option is incorrect because **muscarinic antagonism** is not a mechanism that reduces EPS. Anticholinergic agents are used therapeutically to counteract EPS caused by dopamine blockade, but anticholinergic effects themselves do not prevent or reduce EPS. - The reduction of EPS with atypical antipsychotics is mainly due to **5HT2A antagonism** balancing dopaminergic blockade, selective limbic over striatal binding, and fast D2 dissociation kinetics. *1,4* - This option is incorrect because it omits **5HT2A antagonism**, which is crucial for reducing **negative symptoms** in schizophrenia. - It also incorrectly includes muscarinic antagonism as a mechanism that reduces EPS, when in reality anticholinergics are used to treat EPS rather than prevent it.
Physiology
3 questionsWhich physiological adaptation does not happen at high altitudes?
The countercurrent mechanism is present in which of the following parts of the body? A. Eye B. Testes C. Kidney D. Gut E. Lungs
What does zero pressure indicate in the pressure-volume curve?
INI-CET 2022 - Physiology INI-CET Practice Questions and MCQs
Question 1: Which physiological adaptation does not happen at high altitudes?
- A. Pulmonary vasoconstriction
- B. Respiratory acidosis (Correct Answer)
- C. Hypoxia
- D. Polycythemia
Explanation: ***Respiratory acidosis*** - At high altitudes, the primary physiological response to **hypoxia** is to increase ventilation, leading to a decrease in **arterial PCO2**. - This reduction in **PCO2** causes **respiratory alkalosis**, not acidosis, as the body tries to compensate for the lower oxygen levels. *Pulmonary vasoconstriction* - This is a significant physiological response to **hypoxia** at high altitudes, leading to an increase in **pulmonary artery pressure**. - Its purpose is to divert blood flow to better-ventilated areas of the lung, but it can also contribute to **pulmonary hypertension**. *Hypoxia* - Reduced **atmospheric pressure** at high altitudes directly results in a lower partial pressure of oxygen (**PO2**), leading to **hypoxia**. - This low **PO2** is the primary trigger for most other physiological adaptations seen at high altitudes. *Polycythemia* - Prolonged exposure to **hypoxia** stimulates the kidneys to release **erythropoietin (EPO)**, which in turn increases **red blood cell production**. - This adaptive increase in **red blood cell count** and **hemoglobin concentration** aims to enhance the oxygen-carrying capacity of the blood.
Question 2: The countercurrent mechanism is present in which of the following parts of the body? A. Eye B. Testes C. Kidney D. Gut E. Lungs
- A. A, B, C, D, E are correct
- B. B and C are correct (Correct Answer)
- C. B, C, D, E are correct
- D. A, B, C are correct
Explanation: ***B and C are correct*** - The **countercurrent mechanism** is a biological process where two fluids flow in opposite directions across a semipermeable membrane or in close proximity to maximize exchange efficiency. - **Testes (B)**: The **pampiniform plexus** of veins surrounds the testicular artery, creating a countercurrent heat exchange system. Warm arterial blood descending to the testes is cooled by cooler venous blood ascending from the testes, maintaining the 2-3°C lower temperature required for optimal spermatogenesis. - **Kidney (C)**: The **loop of Henle** and **vasa recta** employ countercurrent multiplication and countercurrent exchange mechanisms to establish and maintain the corticomedullary osmotic gradient, which is essential for concentrating urine. *A, B, C, D, E are correct* - **Eye (A)**: The eye does not have a well-established countercurrent mechanism. Aqueous humor circulation and retinal blood flow do not operate on countercurrent principles. - **Gut (D)**: While intestinal villi have circulation, countercurrent exchange is not a primary or well-established mechanism in standard physiology teaching for the gut. - **Lungs (E)**: The lungs use **concurrent flow**, not countercurrent exchange. Pulmonary capillary blood and alveolar air flow in the same direction, which is less efficient than countercurrent but still allows adequate gas exchange. *A and B are correct* - This option incorrectly includes **Eye (A)**, which does not have a countercurrent mechanism. - It also excludes the **Kidney (C)**, which is one of the most classic and well-taught examples of countercurrent mechanisms in physiology. *A, B, C are correct* - This option incorrectly includes **Eye (A)**, which does not have a countercurrent mechanism. - While it correctly includes testes and kidney, the inclusion of the eye makes this medically inaccurate. *B, C, D, E are correct* - While **Testes (B)** and **Kidney (C)** definitely have countercurrent mechanisms, the inclusion of **Gut (D)** and **Lungs (E)** is incorrect. - The lungs specifically use concurrent, not countercurrent, gas exchange - this is a fundamental concept in respiratory physiology. - Countercurrent exchange in the gut is not a standard teaching point in medical physiology.
Question 3: What does zero pressure indicate in the pressure-volume curve?
- A. Functional residual capacity (Correct Answer)
- B. Inspiratory reserve volume
- C. Tidal volume
- D. Residual volume
Explanation: ***Functional residual capacity*** - This is the lung volume at which the **elastic recoil of the lungs** exactly balances the **elastic recoil of the chest wall**, resulting in zero net pressure across the respiratory system. - At **functional residual capacity (FRC)**, there is no airflow, and the **alveolar pressure equals atmospheric pressure (zero)**, indicating the equilibrium point. - Note: The **transpulmonary pressure remains positive** at FRC (approximately +5 cm H₂O), which keeps the lungs inflated against their elastic recoil. *Inspiratory reserve volume* - This is the **extra volume of air** that can be forcibly inhaled after a normal inspiration. - It involves active inspiration and therefore is associated with a **negative intrathoracic pressure**, not zero pressure. *Tidal volume* - This is the **volume of air inhaled and exhaled** during a normal quiet breathing cycle. - While breathing, pressures fluctuate, and the respiratory system is not at an equilibrium point of **zero pressure** throughout the tidal breath. *Residual volume* - This is the **volume of air remaining in the lungs** after a maximal exhalation. - The chest wall's outward recoil is greater than the lung's inward recoil at this point, resulting in a **negative intrapleural pressure** to keep the lungs from collapsing.
About INI-CET 2022 Questions
This page contains 157 questions from the INI-CET 2022 paper, organised across 19 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the INI-CET exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your INI-CET goals.