INI-CET 2017 — Surgery
9 Previous Year Questions with Answers & Explanations
A car accident patient complains of breathlessness. On examination BP is $110 / 70 \mathrm{mmHg}$ with GCS of 15/15. On examination, trachea is deviated to the right side, with reduced breath sounds in left infra-axillary area and inframammary areas. $S_{1}$ and $S_{2}$ are normal in intensity and splitting. CXR is shown below. What is the best step in management of the patient?

You are asked to put a 22-gauge cannula in a patient. Which of the following cannula will you put?
Which is incorrect about the procedure shown in the patient with right flank pain?

Identify the instrument shown in the image:

Which is correct about hematemesis (upper GI bleeding) in this patient?

What type of choledochal cyst is shown in the image?
Which classification is used to evaluate the condition shown in the image below?

A 30-year-old construction worker had a partial traumatic nail avulsion. 3 weeks later he presents with the presentation shown below. What is the diagnosis?
An HIV positive patient presents with symptoms of toxemia and foul smelling discharge from the lesion shown below. What is the diagnosis?
INI-CET 2017 - Surgery INI-CET Practice Questions and MCQs
Question 1: A car accident patient complains of breathlessness. On examination BP is $110 / 70 \mathrm{mmHg}$ with GCS of 15/15. On examination, trachea is deviated to the right side, with reduced breath sounds in left infra-axillary area and inframammary areas. $S_{1}$ and $S_{2}$ are normal in intensity and splitting. CXR is shown below. What is the best step in management of the patient?
- A. Needle aspiration
- B. Pericardiocentesis
- C. Chest tube insertion (Correct Answer)
- D. Immediate thoracotomy
Explanation: ***Chest tube insertion*** - The patient's symptoms (breathlessness, tracheal deviation to the right, reduced breath sounds in the left infra-axillary and inframammary areas) combined with the CXR findings indicate a **left-sided hemothorax or pneumothorax** causing mediastinal shift. - A chest tube will **drain the accumulated air or fluid**, re-expand the lung, and relieve the mediastinal shift, thereby improving breathing. - This is **NOT a tension pneumothorax** (patient is hemodynamically stable with BP 110/70 mmHg), so definitive chest tube insertion is preferred over needle decompression. *Needle aspiration* - Needle thoracostomy is indicated for **tension pneumothorax**, which presents with hemodynamic instability, severe respiratory distress, and requires immediate decompression. - This patient is **hemodynamically stable** (normal BP, GCS 15/15), indicating a simple pneumothorax or hemothorax that requires **chest tube** for definitive drainage rather than temporary needle aspiration. *Pericardiocentesis* - **Pericardiocentesis** is indicated for **cardiac tamponade**, which presents with muffled heart sounds, hypotension, and distended neck veins (Beck's triad). - The patient's **normal blood pressure, normal heart sounds** (S₁ and S₂ normal), and clinical findings pointing to pleural pathology rule out cardiac tamponade. *Immediate thoracotomy* - **Immediate thoracotomy** is reserved for massive hemothorax with **>1500 mL initial drainage** or **>200 mL/hour persistent bleeding** after chest tube insertion, or for major vessel/cardiac injuries. - Initial management should be **chest tube insertion** for drainage and assessment before proceeding to thoracotomy.
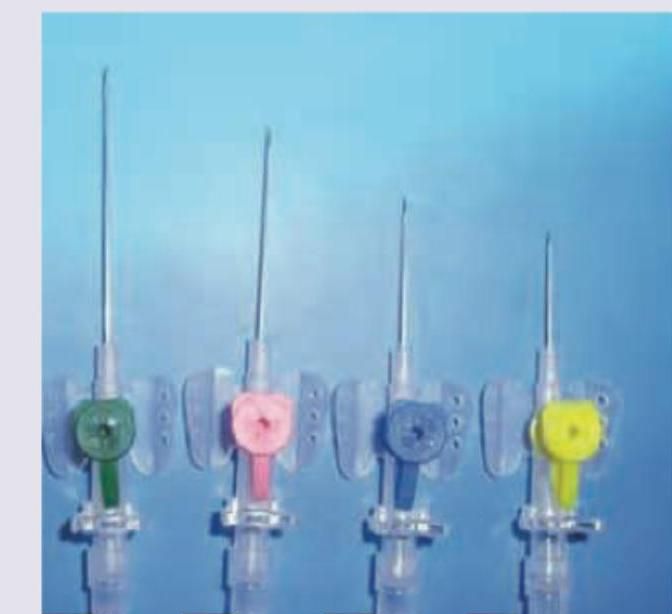
Question 2: You are asked to put a 22-gauge cannula in a patient. Which of the following cannula will you put?
- A. A
- B. C (Correct Answer)
- C. D
- D. B
Explanation: ***C*** - This cannula is blue, which correlates to a **22-gauge** size according to standard color-coding for IV cannulas. - A **22-gauge** cannula matches the specific requirement in the question and is generally used for patients with fragile veins, pediatric patients, or for slow infusions. *A* - This cannula is green, typically indicating an **18-gauge** size. - An 18-gauge cannula provides a larger bore for faster fluid administration but is **too large** for the 22-gauge requirement specified. *B* - This cannula is pink, which corresponds to a **20-gauge** size according to standard color-coding. - A 20-gauge cannula is commonly used for routine infusions but is **larger than the requested 22-gauge** size. *D* - This cannula is yellow, indicating a **24-gauge** size, the smallest common size. - A 24-gauge cannula is **smaller than the requested 22-gauge** and is primarily reserved for very fragile veins and infants.
Question 3: Which is incorrect about the procedure shown in the patient with right flank pain?
- A. No anesthesia is required (Correct Answer)
- B. Done as outpatient procedure
- C. Contraindicated in hard stones
- D. Shockwaves pass through a water bath
Explanation: In the provided image, there is a large, irregularly shaped, radio-opaque density in the right renal area, consistent with a **staghorn calculus**, likely causing the right flank pain. This type of calculus typically fills the renal pelvis and calyces. The question asks what is *incorrect* about the procedure shown, referring to **Extracorporeal Shockwave Lithotripsy (ESWL)**, a common treatment for kidney stones. ***Correct: No anesthesia is required*** - This statement is **incorrect** and is the correct answer to this negation question - ESWL typically requires some form of **analgesia or sedation** (e.g., intravenous fentanyl, midazolam, or even general anesthesia in selected cases) - The shockwaves cause significant discomfort as they are delivered, making **pain management essential** for patient comfort and compliance - While some patients with high pain tolerance may undergo the procedure with minimal analgesia, most require sedation *Incorrect: Contraindicated in hard stones* - This statement is partially correct, making it NOT the best answer - While hard stones (e.g., **calcium oxalate monohydrate, cystine, brushite**) are **more resistant** to ESWL with lower stone-free rates, ESWL is **not absolutely contraindicated** - ESWL can still be attempted for hard stones, though it may require multiple sessions, higher energy settings, or may ultimately fail, necessitating alternative treatments like **ureteroscopy** or **percutaneous nephrolithotomy (PCNL)** - True contraindications include pregnancy, uncorrected bleeding disorders, obstruction distal to the stone, and severe skeletal deformities *Incorrect: Done as outpatient procedure* - This statement is **correct** about ESWL, so it is NOT the answer to this negation question - ESWL is routinely performed on an **outpatient basis**, with patients typically going home the same day - Patients are monitored for a short period post-procedure (usually 1-2 hours) to ensure there are no immediate complications like significant hematuria or pain before discharge - Rarely, patients may require overnight observation if complications arise *Incorrect: Shockwaves pass through a water bath* - This statement is **outdated** but historically accurate - **First-generation ESWL machines** (1980s) utilized a **water bath** in which the patient was partially submerged to couple the shockwaves - **Modern lithotripters** (second and third generation) use a **gel pad** or **water cushion** placed directly on the skin, eliminating the need for water immersion while maintaining acoustic coupling - While technically incorrect for modern ESWL, the statement was historically true, making "no anesthesia required" a more definitively incorrect statement
Question 4: Identify the instrument shown in the image:
- A. Asepto syringe (Correct Answer)
- B. Trocar for tapping hydrocele
- C. Czerny retractor
- D. Malecot catheter
Explanation: ***Asepto syringe*** - The image displays a **red rubber bulb** attached to a glass or plastic barrel ending in a nozzle, which is characteristic of an **Asepto syringe**. - Asepto syringes are commonly used for **irrigation** of wounds or surgical sites, and for various procedures where precise suction or fluid delivery is needed without a needle. *Trocar for tapping hydrocele* - A **trocar** is a pointed medical instrument with a sharp tip, typically used with a cannula to introduce instruments or drain fluids from a body cavity. - Trocars for hydrocele tapping would differ significantly in appearance, featuring a pointed tip and often a stylet, which are absent here. *Czerny retractor* - A **Czerny retractor** is a surgical instrument with two blades, used primarily to hold back tissue during surgery to provide a clear view of the surgical field. - The instrument shown here is focused on fluid suction/delivery, not on tissue retraction. *Malecot catheter* - A **Malecot catheter** is a type of self-retaining catheter, typically made from soft, flexible material, with a distinctive mushroom-shaped tip that helps anchor it within a viscus. - This image clearly depicts a syringe-like device with a bulb, not a flexible catheter with a four-winged tip.
Question 5: Which is correct about hematemesis (upper GI bleeding) in this patient?
- A. Most common is variceal bleeding
- B. Occurs only if bleeding occurs proximal to ligament of Treitz
- C. MC management is endoscopic banding
- D. Rockall scoring is used for risk stratification (Correct Answer)
Explanation: ***Rockall scoring is used for risk stratification*** - The image shows a patient with significant **hematemesis**, indicating an upper gastrointestinal bleed. The **Rockall score** is a validated tool used to assess the risk of rebleeding and mortality in patients with upper GI bleeding. - This scoring system considers factors such as **age**, **shock**, **comorbidity**, and endoscopic findings to guide management. *Most common is variceal bleeding* - While variceal bleeding is a serious cause of upper GI hemorrhage, **peptic ulcer disease** (gastric or duodenal ulcers) is the most common cause of non-variceal upper GI bleeding, accounting for 40-50% of cases. - Variceal bleeding is common in patients with **portal hypertension**, often due to liver cirrhosis. *Occurs only if bleeding occurs proximal to ampulla of Vater* - **Hematemesis** (vomiting blood) specifically indicates bleeding **proximal to the ligament of Treitz**, which is superior to the ampulla of Vater. - Bleeding from the small intestine distal to the ligament of Treitz or the colon typically results in **melena** or **hematochezia**, not hematemesis. *MC management is endoscopic banding* - **Endoscopic banding** is the primary treatment for **esophageal variceal bleeding**. - For non-variceal bleeding, such as from **peptic ulcers**, the most common endoscopic management is **epinephrine injection** followed by **thermal coagulation** or **clip placement**.
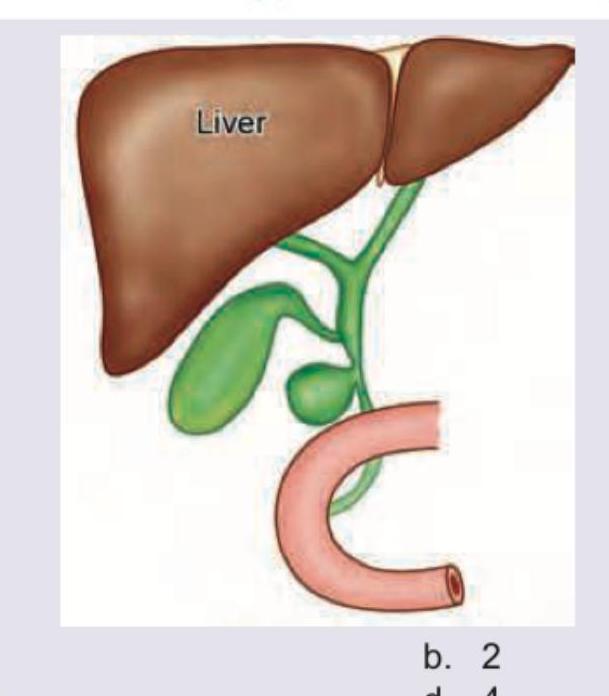
Question 6: What type of choledochal cyst is shown in the image?
- A. 1
- B. 2 (Correct Answer)
- C. 3
- D. 4
Explanation: ***2*** - The image displays a **diverticulum** protruding from the side of the **common bile duct (CBD)**, which is characteristic of a **Type II choledochal cyst**. - Type II choledochal cysts are rare, focal diverticula of the CBD, typically managed by excision. *1* - Type I choledochal cysts involve **fusiform or cystic dilation** of the extrahepatic bile duct, not a diverticulum protruding from the side. - They are the most common type and are usually treated with cyst excision and Roux-en-Y hepaticojejunostomy. *3* - Type III choledochal cysts, also known as **choledochoceles**, involve **dilation of the intraduodenal portion** of the CBD. - This typically appears as an intraduodenal cyst, which is not depicted in the image. *4* - Type IV choledochal cysts involve **multiple dilations** of the intrahepatic and/or extrahepatic bile ducts. - The image shows a single diverticular outpouching, not multiple dilations.
Question 7: Which classification is used to evaluate the condition shown in the image below?
- A. Todani classification (Correct Answer)
- B. Bismuth classification
- C. Johnson classification
- D. Maastricht classification
Explanation: ***Todani classification*** - The image provided shows an **ERCP (Endoscopic Retrograde Cholangiopancreatography)** with contrast in the biliary tree, demonstrating a dilated common bile duct (CBD) marked with an arrow. This appearance is characteristic of a **choledochal cyst**. - The **Todani classification** is a widely used system for categorizing choledochal cysts, which are congenital dilations of the biliary tree. *Bismuth classification* - The Bismuth classification is used to categorize **cholangiocarcinomas** (cancers of the bile ducts), particularly those affecting the hepatic confluence (Klatskin tumors). - It describes the extent of involvement of the hepatic duct bifurcation, which is distinct from the diffuse or localized dilations seen in choledochal cysts. *Johnson classification* - The Johnson classification is used for categorizing **duodenal ulcers**, specifically related to their location within the duodenum (e.g., gastric acid hypersecretion vs. normal acid production). - This classification is entirely unrelated to biliary tree pathologies. *Maastricht classification* - The Maastricht classification is used for grading **hepatic encephalopathy**, which is a neuropsychiatric complication of liver failure. - It describes the severity of neurological symptoms in patients with liver disease and has no relevance to imaging findings of biliary anomalies.
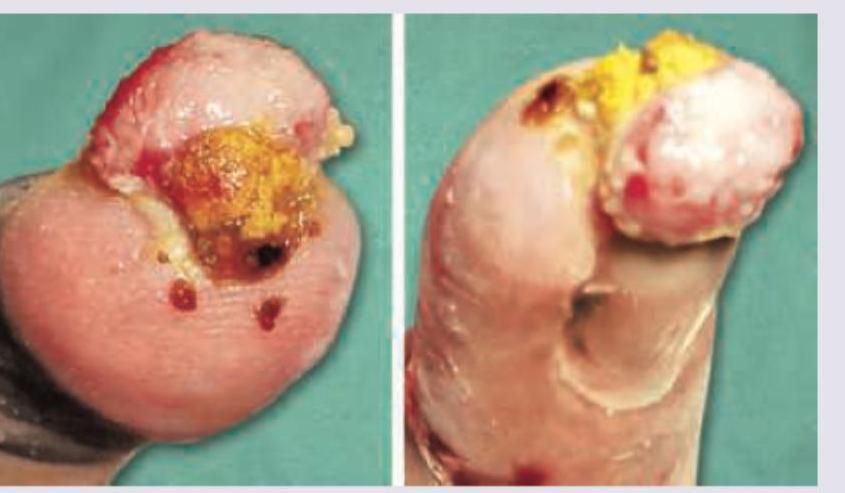
Question 8: A 30-year-old construction worker had a partial traumatic nail avulsion. 3 weeks later he presents with the presentation shown below. What is the diagnosis?
- A. Pyoderma gangrenosum
- B. Pott's puffy tumor
- C. Pyogenic granuloma (Correct Answer)
- D. Acute paronychia
Explanation: ***Pyogenic granuloma*** - The image shows a **fleshy, red, often ulcerated nodule** following a partial traumatic nail avulsion, which is highly characteristic of a pyogenic granuloma. - These lesions are **reactive vascular proliferations** that typically develop rapidly at sites of trauma or inflammation. *Pyoderma gangrenosum* - Pyoderma gangrenosum characteristically presents as a rapidly enlarging, painful **ulcer with violaceous undermined borders** and often a purulent base, which differs from the described lesion. - It is typically associated with **systemic diseases**, such as inflammatory bowel disease or hematologic malignancies, and does not typically present as a focal, exophytic growth after localized trauma. *Pott's puffy tumor* - Pott's puffy tumor is a subperiosteal abscess of the frontal bone, usually caused by sinusitis, leading to a **forehead swelling** with osteomyelitis and epidural abscess. - This condition involves the **skull** and brain, not the nail bed, and presents with different clinical features like fever, headache, and periorbital edema. *Acute paronychia* - Acute paronychia is an **infection of the nail fold**, presenting with pain, redness, and swelling around the nail, often with pus accumulation. - While it can follow minor trauma, it is characterized by **inflammatory signs of infection** in the paronychial area, not a rapidly growing, exuberant granulation-like tissue as shown.
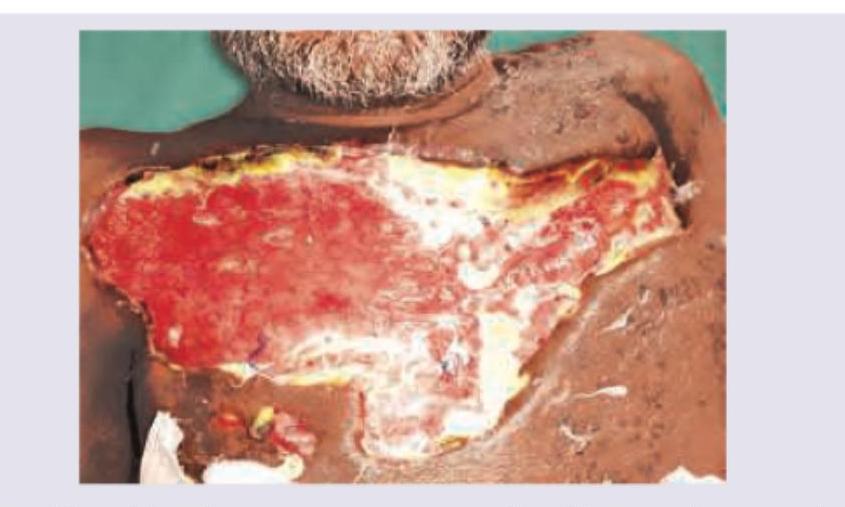
Question 9: An HIV positive patient presents with symptoms of toxemia and foul smelling discharge from the lesion shown below. What is the diagnosis?
- A. Trophic ulcer
- B. Pyogenic granuloma
- C. Martorell ulcer
- D. Necrotizing fasciitis (Correct Answer)
Explanation: ***Necrotizing fasciitis*** - The image shows an extensive, deep soft tissue infection with a large area of **tissue necrosis**, which is characteristic of necrotizing fasciitis. - The patient's **HIV-positive status** puts them at higher risk for severe infections, and the symptoms of **toxemia** and **foul-smelling discharge** further support this aggressive, rapidly spreading bacterial infection. *Trophic ulcer* - Trophic ulcers are typically caused by **neuropathic or vascular insufficiency**, leading to chronic, poorly healing wounds, often located on the lower limbs. - They do not usually present with the rapid onset, extensive tissue destruction, toxemia, and foul-smelling discharge seen here. *Pyogenic granuloma* - A pyogenic granuloma is a **benign vascular lesion** that typically presents as a small, red, rapidly growing, pedunculated or sessile papule, prone to bleeding. - It does not involve widespread tissue destruction, toxemia, or a foul-smelling discharge. *Martorell ulcer* - A Martorell ulcer (or ischemic hypertensive leg ulcer) is a **painful, full-thickness ulcer** typically located on the lateral aspect of the lower leg, associated with poorly controlled **hypertension and peripheral arterial disease**. - While it is an ulcer, it doesn't typically present with the broad, necrotizing appearance, toxemia, or foul-smelling discharge indicative of such a severe, spreading infection.