INI-CET 2017 — Pediatrics
3 Previous Year Questions with Answers & Explanations
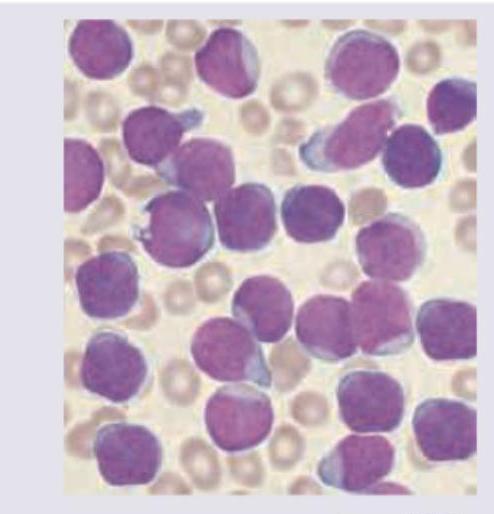
A 7-year-old boy presents with fever and weight loss. On examination he had pallor with lymphadenopathy. Peripheral smear is shown below. Diagnosis is: (AIIMS May 2017)
Comment on the diagnosis of the image shown below. (AIIMS Nov 2017)

The image shows:

INI-CET 2017 - Pediatrics INI-CET Practice Questions and MCQs
Question 1: A 7-year-old boy presents with fever and weight loss. On examination he had pallor with lymphadenopathy. Peripheral smear is shown below. Diagnosis is: (AIIMS May 2017)
- A. ALL (Correct Answer)
- B. AML
- C. Aplastic anemia
- D. Juvenile myelomonocytic leukemia
Explanation: ***ALL*** - The peripheral smear shows numerous **blasts** with **scanty cytoplasm**, **prominent nucleoli**, and a **high nuclear-to-cytoplasmic ratio**, which is characteristic of **acute lymphoblastic leukemia (ALL)**. - Clinical features such as **fever**, **weight loss**, **pallor**, and **lymphadenopathy** in a 7-year-old child are classic presentations of ALL, the most common childhood leukemia. *AML* - While AML also presents with acute symptoms and blasts, the blasts in AML typically have **more abundant cytoplasm**, and may contain **Auer rods**, which are not clearly visible here. - The **morphology of the blasts** in the image, with their uniformly high N/C ratio and immature appearance, points away from typical AML. *Aplastic anemia* - Aplastic anemia is characterized by **pancytopenia** in the peripheral blood and **hypocellular bone marrow**, meaning a significant reduction in all blood cell lines, and **lacks the presence of blasts**. - The image clearly displays a proliferation of immature cells (blasts), which is contrary to the pathology of aplastic anemia. *Juvenile myelomonocytic leukemia* - JMML is a rare disorder characterized by **monocytosis**, **splenomegaly**, and typically presents in very young children (median age 2 years), often with **rashes** and **adenopathy**. - While there is some overlap in symptoms, the predominant cell type in the smear does not suggest a significant monocytic component, and the clinical picture in a 7-year-old child is less typical for JMML without other defining features.
Question 2: Comment on the diagnosis of the image shown below. (AIIMS Nov 2017)
- A. Hypothyroidism (Correct Answer)
- B. Hyperthyroidism
- C. Sarcoidosis
- D. Diabetes
Explanation: ***Hypothyroidism*** - The image depicts **myxoedema**, characterized by localized, non-pitting edema and thickened skin, typically on the shins, which is a classic manifestation of severe **hypothyroidism**. - This condition results from the accumulation of **hyaluronic acid** and chondroitin sulfate in the dermis, causing a characteristic doughy texture. *Hyperthyroidism* - While hyperthyroidism (specifically Graves' disease) can cause **pretibial myxoedema**, the image alone showing generalized myxoedematous changes is more indicative of **hypothyroidism**. - Pretibial myxoedema associated with hyperthyroidism typically presents as elevated, firm, non-pitting plaques, whereas the image shows a more widespread thickening. *Sarcoidosis* - Sarcoidosis involves the formation of **non-caseating granulomas** in various organs, including the skin. - Skin manifestations of sarcoidosis can include **erythema nodosum**, plaques, or lupus pernio, which do not match the generalized thickening seen in the image. *Diabetes* - Diabetes mellitus can cause various skin manifestations such as **diabetic dermopathy**, necrobiosis lipoidica diabeticorum, and acanthosis nigricans. - These conditions present with different visual characteristics, like hyperpigmented atrophic macules or waxy yellow plaques, unlike the diffuse thickening shown.
Question 3: The image shows:
- A. Bladder exstrophy (Correct Answer)
- B. Urachal anomalies
- C. Systolic bladder
- D. Congenital adrenal hyperplasia
Explanation: ***Bladder exstrophy*** - The image clearly displays an **exposed bladder mucosa** projecting from the lower abdominal wall, which is characteristic of bladder exstrophy. - This congenital anomaly results from a **failure of fusion of the anterior abdominal wall** and bladder during embryonic development. *Urachal anomalies* - Urachal anomalies involve persistent remnants of the **urachus**, connecting the bladder to the umbilicus, leading to cysts, sinuses, or fistulas. - They typically appear as lesions at or near the **umbilicus** and do not involve the direct exposure of the bladder. *Systolic bladder* - "Systolic bladder" is **not a recognized medical term** for a congenital anomaly. - Bladder function is described in terms of contraction (systole) and relaxation (diastole) but does not refer to a structural malformation. *Congenital adrenal hyperplasia* - This is an **endocrine disorder** affecting hormone production by the adrenal glands, leading to ambiguous genitalia in some cases. - It does not involve a **visible external defect of the bladder** or abdominal wall.